

Abstract
Background
Limited research has examined how the functions of self-injurious behaviour (SIB) relate to the production of injuries and the location, type or severity of those injuries.
Methods
Clinical and medical records were coded for 64 individuals hospitalised for SIB. When injuries were present, the physical properties of SIB and injuries were assessed across groups of individuals with automatically and socially maintained SIB.
Results
Injuries were observed for 35 of the individuals who engaged in SIB. Individuals who engaged in a single form of SIB were more likely to have injuries (P < .05). Individuals with SIB maintained by automatic reinforcement had significantly more severe injuries to the head than those in the social group (q < .05, P = .0132, H = 12.54).
Conclusion
Although results are preliminary, the results provide evidence that the function of SIB may influence the severity and location of injuries produced.
Keywords: automatic reinforcement, functional analysis, injury, self-injurious behavior, social reinforcement
Introduction
Self-injurious behaviour (SIB) occurs in approximately 5% to 41% of individuals diagnosed with intellectual and developmental disabilities (IDD; Cooper et al. 2009; Soke et al. 2016). Although SIB may be a very persistent response across an individual’s lifetime (Emerson et al. 2001), some acts or patterns of SIB may be more or less dangerous based on the injuries they produce. For example, forceful headbanging to the corner of a kitchen counter is likely to produce both immediate and serious lacerations and contusions; whereas scratching the palm of the hand will likely require many instances before an abrasion occurs. Hyman et al. (1990) demonstrated this wide range of injuries produced by SIB (SIB-related injuries) in 97 individuals who were admitted for a brief hospital stay to treat SIB. Of these individuals, 75 were reported to have SIB-related injury, which varied from very minor (e.g. superficial scratches) to very severe (e.g. tooth fractures, bone fractures and retinal detachment).
The behavioural treatment literature spanning over three decades shows that function (the maintaining variable or variables of the behaviour) is a critical dimension of SIB and that the most effective treatments for SIB are those that are designed specifically to address that function (e.g. Iwata et al. 1994; Herzinger & Campbell 2007). Functional analysis (FA) of problem behaviour (Iwata et al. 1982) is currently considered best practice for identifying the function of SIB (Kahng et al. 2015). The functions of SIB, as determined in an FA, are divided into two broad classes: socially reinforced SIB (i.e. the reinforcer for SIB is mediated by another person) and automatically reinforced SIB (i.e. the reinforcer for SIB is not mediated by another person). In approximately 75% of cases, SIB is socially reinforced, meaning it can be occasioned and maintained by social variables, most commonly attention, access to preferred items and escape; whereas in approximately 25% of cases, SIB is automatically reinforced (Beavers et al. 2013; Iwata et al. 1994). The term ‘automatic’ reinforcement is used to describe SIB that occurs independent of social variables because it is presumed that the occurrence of SIB produces reinforcement directly via a biological process. Potential sources of automatic reinforcement produced by SIB include access to sensory stimulation (Goh et al. 1995), production of opioids (Thompson et al. 1995) and pain attenuation (Kennedy & Thompson 2000). However, it is unknown if or how the function of SIB affects the form of SIB and location, type or severity of SIB-related injuries.
Research on SIB presumed or shown to be automatically maintained provides some evidence to suggest that at least some physical properties of SIB may be related to its function. A few studies have catalogued SIB sites, as preference for engaging in SIB at particular body sites may provide insight into the biological conditions that occasion and maintain SIB. Symons and Thompson (1997) examined the body SIB sites for 29 individuals with IDD. The authors found that 32% of SIB sites were associated with body sites known to be important for the production of analgesia when electrically or mechanically stimulated. Wisely et al. (2002) subsequently replicated this finding for 53 individuals. Relatedly, Breau et al. (2003) found differences in the amount of body surface targeted and the total number of SIB sites for children with and without chronic pain. Although these studies do not present direct data on SIB-related injuries, location of injury sites should be a product of SIB sites; thus, injuries could also be related to the underlying function of SIB.
One study has documented injuries for individuals shown to have automatically reinforced SIB. Hall et al. (2014) examined several aspects of SIB for 13 individuals diagnosed with Prader–Willi syndrome. Although the purpose of the study was to better characterise SIB in individuals with Prader–Willi syndrome, SIB was found to be automatically reinforced in all conclusive assessment outcomes. In addition, the authors collected data on observed injuries using the Self-Injury Trauma scale (SIT scale; Iwata et al. 1990). Based on the scores on the SIT scale, an ‘estimated current risk’ associated with SIB was calculated for each individual. Hall et al. found that SIB was automatically reinforced for eight individuals, and of these eight individuals, the SIT scale determined high injury risk associated with SIB in six of eight cases. For the remaining five individuals, the function of SIB could not be determined.
As previously noted, function plays an important role in the occurrence of SIB. By definition, the events that occasion and maintain SIB are different across functional classes. However, there is reason to suspect that the physical form of SIB, and hence subsequent injury incurred from SIB, may also be different for automatically and socially reinforced SIB. In particular, because automatically reinforced SIB presumably produces an internal event, it is reasonable to suspect that reliable access to that internal event may require more invariant forms of SIB. Whereas, because socially reinforced SIB occurs to access a reinforcer that is mediated by another individual, it is reasonable to suspect that the form of SIB adapts to the particular audience providing the reinforcer. Thus, it is possible that differences in the number of injury locations and the degree of injury severity may be present across these groups. A comparative analysis of injuries in individuals with automatically reinforced and socially reinforced SIB has never been conducted. However, better understanding of the risk of injuries as related to functional classes of SIB may assist in identifying the mechanisms supporting automatically reinforced SIB and would be a preliminary step in allowing for prescription of treatment intensity (especially triage care when catastrophic injuries are imminent). Thus, the primary purpose of the current study was to classify the physical properties of SIB and injuries across groups of individuals with SIB that was or was not automatically reinforced. Secondarily, we provide descriptive information on individuals who engage in SIB who did and did not have injuries.
Methods
Ethical approval
Prior to initiating this study, a protocol describing the study was submitted to the Kennedy Krieger Institute and the Johns Hopkins University School of Medicine internal review boards by the first author. These boards approved the study protocol as outlined in the succeeding text.
Study design and participants
A consecutive case series and record review was conducted of individuals admitted to a hospital unit that specialised in the treatment of SIB from 2004 to 2015. Cases were screened to determine if the following sources of data were available and complete: (1) clinical discharge summaries and records that indicated that the individual engaged in SIB that had been assessed in an FA, (2) report of physical examination conducted at the time of admission and (3) FA data that were interpretable using the criteria outlined by Hagopian et al. (1997) and Roane et al. (2013). The final step was included because the function of SIB was directly related to the purpose of the study, and the use of structured criteria ensured that the function determined was based on an objective and replicable standard.
We initially identified 134 individuals who had clinical discharge summaries and records that indicated they engaged in SIB (criterion 1). However, the additional inclusion criteria were not met for 70 individuals. For 62 of these individuals, a physical examination was not found (criterion 2); for the remaining eight individuals, the FA was not interpretable (criterion 3). Thus, the records for 64 individuals were retained.
Data sources and collection
Review of clinical discharge summaries
The discharge summaries were coded by the third author to identify individual demographic data.
Review of functional analysis descriptions and interpretation
The purpose of the FA was to determine the function of SIB by comparing the level of SIB1 in specific test conditions with the level of SIB in a control condition. The progressive model of FA described in Hagopian et al. (2013) was standard practice to assess the function of SIB for all individuals. This progressive model typically began with a ‘standard’ FA and then advanced to individualised analysis (e.g. pairwise analysis of a particular test condition) at the discretion of the overseeing Board Certified Behavior Analyst. The standard FA was conducted in a manner similar to that described by Iwata et al. (1982) and typically included three to four test conditions, as well as a control condition. Common test conditions included Alone (or No interaction), Attention, Demand and Tangible conditions.
In the Alone (or No interaction) condition, the individual was alone in a room (or in a room with a therapist who ignored him or her), and no programmed consequences were provided when SIB occurred. This condition was used to test if SIB persisted in the absence of consequences, which would suggest SIB was automatically reinforced. In the Attention condition, the individual was in a room with the therapist, who ignored the individual; if SIB occurred, the therapist provided the individual with brief vocal and physical attention. This condition was used to test if SIB was socially reinforced by access to attention. In the Demand condition, the individual was in a room with the therapist, who asked the individual to complete common tasks; if SIB occurred, the therapist halted demand presentation for a brief period. This condition was used to test if SIB was socially reinforced by escape from task demands. In the Tangible condition, the individual was in a room with the therapist, who restricted access to a food or leisure item; if SIB occurred, the therapist provided access to the item (either a small amount of food or brief access to the leisure item). This condition was used to test if SIB was socially reinforced by access to tangible items. In all cases, the level of SIB in the test conditions was compared with the level of SIB in the Play (control) condition, in which the individual was in a room with a therapist who freely provided preferred leisure items and attention, and ignored SIB. Additional analyses conducted following the initial standard FA incorporated some variation on this FA methodology.
As noted earlier, FA data were analysed using a modified version of the structured criteria for interpretation of FA data developed by Hagopian et al. (1997) and further refined by Roane et al. (2013).2 After the function(s) of SIB was determined, individuals were sorted into groups based on the presence or absence of SIB maintained by automatic reinforcement. That is, individuals having at least one topography of SIB maintained by automatic reinforcement were sorted to the automatic group and individuals with SIB exclusively maintained by social variables and with no topographies of SIB maintained by automatic reinforcement of SIB were sorted to the social group.
Each FA description was coded to determine the specific forms of SIB that were assessed (e.g. hand to head punching). That is, for each individual, the forms of SIB were coded as (1) ‘sharp’ SIB if the contact between body parts included either nails or teeth (this included self-biting, pinching and scratching); or (2) ‘blunt’ SIB, if the contact did not involve nails and teeth but was between other body parts or body parts and the environment (this included body-hitting, body to surface, self-kicking, headbanging, head-hitting, object to head, shoulder to head and knee to head).
As a final step, in order to compare the occurrence of SIB across groups, data on the responses per minute (rate) of SIB in the FA play condition were gathered. The rate of SIB in the play condition was selected because (1) all individuals experienced this condition in the FA and (2) in the play condition, there are no changes to the antecedent and consequent events based on the occurrence of SIB (i.e. SIB was neither encouraged or discouraged). We calculated the average rate of SIB across all FA play sessions in FAs where a function was identified for each individual. Two individuals (one in the automatic group and one in the social group) were excluded from this analysis because of particular aspects of their FAs.3
Review and scoring of physical examinations
At intake, registered nurses, who had been trained to work with the population, completed physical examinations, which included descriptions of any injuries. These written records served as the data on injuries. Each individual’s records from the physical examination were coded in terms of their number of injury sites, location of injury sites, type of injuries and severity of injuries, similar to the categories outlined in the SIT scale (Iwata et al. 1990). Injuries were classified across the following dimensions:
Frequency of injuries: For each individual, we counted the number of injury sites across the body. Unfortunately, the number of injuries at a particular body area was often not reported in physical exams, so we did not retain this information for any individual. For example, the physical examination might report an injury to the hand but not the exact number of injuries on the hand. Thus, although injuries at different sites were reported (e.g. left shoulder and right hand) for an individual, it was not possible to identify the number of injuries within a specific site (e.g. the right hand).
Location of injuries: We collected data on the location of each injury using the segments of the body described in the SIT scale. Subsequently, we condensed data into three broad categories (head, torso and extremities) to produce summative data, as these are the general categories described in the SIT scale. Injuries to the head included any injury to the neck or above; injuries to the torso included any injury below the neck and not including arms, hands, legs and feet; injuries to the extremities included any injury to the arms, hands, legs or feet.
Type of injuries: Injuries were coded as abrasions and lacerations, which are breaks in the skin, and contusions, which are distinct areas marked by abnormal discolouration or swelling.
Severity of injuries: Finally, the severity of that injury was scored based on the type of injury (as outlined by the SIT scale). Injuries of each type were scored as mild tissue damage (=1), moderate tissue damage (=2) or severe tissue damage (=3), using the definitions described by Iwata et al. (1990).
In order to assess the reliability of these data collection procedures, the third author and another individual independently coded physical examinations using this procedure for 16 cases. Based on these data, a single rating, absolute agreement, two-way mixed effect interclass correlation coefficient (Koo & Li 2016) was calculated on the frequency of injury locations reported (range 1–8 injury sites), the location of these injuries (the head, torso and extremities), the type of these injuries (abrasion/laceration, contusion or neither type of injury) and severity of injuries (no tissue damage, mild tissue damage, moderate tissue damage or severe tissue damage). Results of this analysis were calculated using GraphPad Prism 6 (GraphPad Software, Inc., La Jolla, CA, USA) and Microsoft Excel version 2010 (Microsoft Corp., Redmond, WA, USA). For frequency of injuries, intraclass correlation (ICC) was .79 with a 95% confidence interval of .54 to .93; for location of injuries, ICC was .82 with a 95% confidence interval of .72 to .91; for type of injuries, ICC was .99 with a 95% confidence interval of .99 to 1; for severity of injuries, ICC was .99 with a 95% confidence interval of .99 to 1.
Statistical methods
For the comparison of individuals with and without injuries, due to the small sample size, we used nonparametric statistics to compare the rate of SIB across Play conditions, as well as differences in the forms, and number of forms of SIB. Finally, we compared the proportion of individuals who had an injury based on the function of their SIB (automatic or socially reinforced). For the individuals with injury, due to the relatively small sample size, and because less than 10 injuries were recorded across some injury outcome measures (e.g. torso injuries), we used nonparametric statistics adjusting for multiple comparisons to examine SIB and injury variables across groups of individuals with automatically and socially reinforced SIB. In doing so, we conducted posttests that controlled for the false discover rate (FDR) using two-stage linear step-up procedure (Benjamini et al. 2006). These statistical tests were completed using GraphPad Prism 6 (GraphPad Software, Inc.). Because injuries to the head have been considered a greater risk in previously published research on injuries (e.g. Iwata et al. 1990), we also examined differences in the severity of head injuries in comparison with other injuries. We did not assess the rate of SIB across automatically and socially reinforced SIB groups because the rate of SIB in the play condition was directly related to group assignment in some cases (i.e. an elevated level of responding is characteristic of automatically reinforced SIB in some cases; Iwata et al. 1994).
Results
Comparison of self-injurious behaviour properties
Table 1 shows the demographic characteristics for all 64 individuals that met the inclusion criteria. Of the 64 individuals, 35 individuals were determined to have at least one physical injury present during their intake physical examination; 29 were reported to engage in SIB but did not have a physical injury present during their intake physical examination.
Table 1.
Demographic information across groups of individuals with and without injuries, as well as automatically and socially reinforced self-injury
| All individuals |
Individuals with injuries |
|||||
|---|---|---|---|---|---|---|
| All | Automatic | Social | All | Automatic | Social | |
| Number | 64 | 32 | 32 | 35 | 18 | 17 |
| Age | ||||||
| Children (5–11) | 26 | 13 | 13 | 16 | 7 | 9 |
| Adolescents (11–17) | 25 | 13 | 12 | 14 | 10 | 4 |
| Adults (>18) | 13 | 6 | 7 | 5 | 1 | 4 |
| Gender | ||||||
| Female | 20 | 11 | 9 | 11 | 8 | 3 |
| Male | 44 | 21 | 23 | 24 | 10 | 14 |
| Level of ID | ||||||
| Mild–Moderate | 15 | 10 | 5 | 6 | 5 | 1 |
| Severe–Profound | 22 | 10 | 12 | 13 | 6 | 7 |
| Unspecified | 15 | 8 | 7 | 8 | 5 | 3 |
| Unknown | 12 | 4 | 8 | 8 | 2 | 6 |
| ASD | ||||||
| Yes | 58 | 29 | 29 | 30 | 16 | 14 |
| No | 6 | 3 | 3 | 5 | 2 | 3 |
ASD = Autism Spectrum Disorder.
Across the groups with and without injury, no significant difference in the rates of SIB in the play condition was observed; in fact, across groups with and without injury, the mean rate and standard deviation of the rate were very similar (mean ~1.3; SD ~2.7). However, a difference between the groups was observed as related to the form of the behaviour. As seen in Table 2, injury was significantly more likely when individuals engaged in a single form of SIB (injury present in 77.8% of individuals) rather than multiple forms of SIB (injury present in 45.6% of individuals) using Fishers exact test (P < .05).
Table 2.
Number of individuals with specific forms of self-injurious behaviour across groups of individuals with and without injuries, as well as automatically and socially reinforced self-Injury
| Single form |
|||||
|---|---|---|---|---|---|
| Individuals | Sharp | Blunt | Total | Multiple forms (sharp and blunt) Total | |
| Without injury | 29 | 0 | 4 | 4 | 25 |
| Automatic | 14 | 0 | 2 | 2 | 12 |
| Social | 15 | 0 | 2 | 2 | 13 |
| With injury | 35 | 2 | 12 | 14 | 21 |
| Automatic | 18 | 0 | 8 | 8 | 10 |
| Social | 17 | 2 | 4 | 6 | 11 |
Across functional classes, a similar proportion of individuals with injury had automatically (56.3%) and socially reinforced SIB (53.1%). Individuals in the social group were more likely to engage in exclusively sharp SIB, and individuals in the automatic group were more likely to engage in exclusively blunt SIB. However, the majority of individuals in both groups engaged in both sharp and blunt SIB. As noted earlier, a rate analysis was not conducted across these groups.
Comparison of injury properties across automatic and social groups
Injury characteristics:
When comparing each injury variable in isolation (total number of injuries, total number of injuries across locations of injury site, total number of each type of injury and the mean severity of injuries across injuries), the automatic and social groups did not differ markedly on any single injury variable. Individuals had almost an identical frequency of injury sites, a similar distribution of locations of injury sites, a similar proportion of injury types and no difference in injury severity across all sites. Because this is the most general level of analysis, we also examined the interaction of injury variables.
Combined injury characteristics
Only minor and insignificant differences were found when assessing group differences by location of injury site and type of injury, as well as when assessing group differences by injury severity and type of injury; thus, these data are not presented. However, a number of interesting findings emerged when assessing group differences by location of injury sites and severity of injuries.
Comparing groups by location of injury site and severity of injury revealed the most robust differences between automatic and social groups. Individuals in the automatic group were more likely to have more severe injuries to the head; individuals in the social group were more likely to have more severe injuries to the torso; and individuals in both groups were highly likely to have mild injuries to the extremities. However, the most severe injuries to the extremities occurred exclusively in the social group. Figure 1 shows all 90 injuries in each group with the location of each injury site, as well as the severity of those injuries. Further, for additional information on the severity of injury at each body site for each individual can be seen in Figure S1. Given the differences observed across location of injury sites and severity of injury observed, additional analysis was conducted on these two variables. Because mild injuries may be less concerning, and because head injuries have been considered more risky in previous research (e.g. Iwata et al. 1990), we assessed the proportion of individuals who had a moderate to severe injuries to the head vs. injuries to the torso and extremities. A greater proportion of individuals in the automatic group had these types of injury to the head (55.5% in comparison with 23.5% in the social group); whereas a greater proportion of individuals in the social group had these types of injuries to the body and extremities (41.8% in comparison with 11.1% in the automatic group). Although these groups are small, this difference was found to be significant using a Fisher’s exact test (P < .05).
Figure 1.
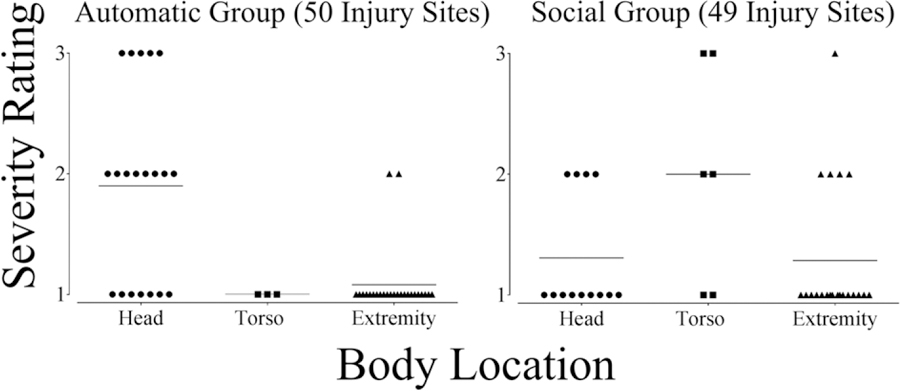
All injuries across groups, separated by location sites and severity of injury.
In addition, Figure 2 shows the single most severe injury to the three body sites for any individual with a moderate or severe injury to that body site, as well as the injury type across groups. For one individual in the automatic group, an abrasion/laceration and contusion were scored as equal severity to the head. Interestingly, the most severe injuries to the head were only observed in the automatic group, and these were all contusions. In contrast, the most severe injuries to the torso and extremities were only found in the social group, and these were all abrasions/lacerations.
Figure 2.
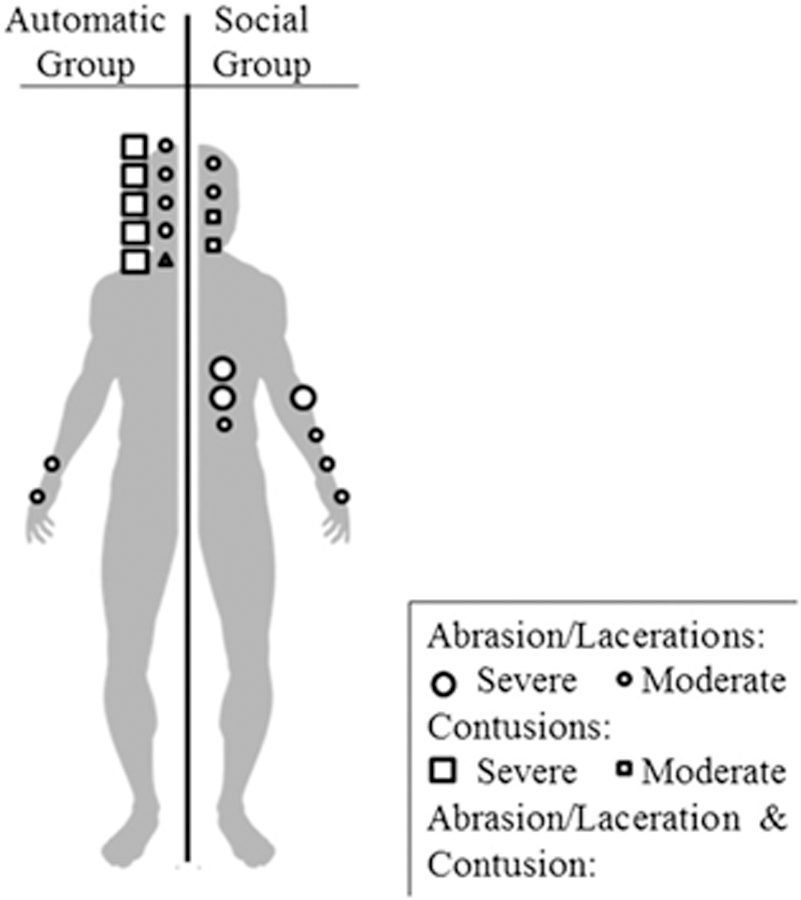
Location of injury site and type of each individual’s most severe injury, for all individuals with at least one moderate or severe injury at that body site. Injuries are presented across automatic (left) and social group (right).
Based on the observed difference in the percentage of individuals with injuries to the head and the torso or extremities, additional statistical analysis was conducted on the most severe injury for each individual who had an injury at those locations across groups. That is, the severity rating of the most severe injury for the 12 individuals in the automatic group with a head injury, the 11 individuals in the automatic group with a torso or extremity injury, 10 individuals in the social group with a head injury and the 13 individuals in the social group with a torso or extremity injury were analysed. A Kruskal–Wallis test was conducted comparing the most severe injury to the head and to the torso/extremities across individuals in the automatic and social groups; this included a posttest incorporating the FDR. Results indicated a significant difference across groups, and the posttest revealed a significant difference in the severity of head wounds for individuals in the automatic and social group (q < .05, P = .0132, H = 12.54) and the severity of injuries at different locations for the automatic group (q < .05, P = .0008, H = 12.54). Specifically, the average severity of ratings for the automatic group’s head injuries was greater, 2.3 (SD = 0.8; range of scores 1–3), than the average severity in the social group, 1.4 (SD = 0.5; range of scores 1–2). In addition, head injuries in the automatic group were more severe than torso or extremity injuries in this group, which had an average severity of 1.2 (SD = 0.4; range of 1–2). Although there was no significant difference in torso and extremity wounds across groups, the social group tended to have more severe injuries at these locations (M = 1.8, SD = 0.8, range 1–3) than the automatic group (M = 1.2, SD = 0.4, range 1–2).
The prior analysis combined torso and extremity injuries based on the premise that head injuries have been considered more dangerous by some (e.g. Iwata et al. 1990), but very few individuals had torso injuries (two individuals in the automatic group and four individuals in the social group), and similar results were obtained directly comparing head and extremity injuries. When comparing the severity rating of the most severe injury for the 12 individuals in the automatic group with a head injury, the 10 individuals in the automatic group with an extremity injury, 10 individuals in the social group with a head injury and the 12 individuals in the social group with an extremity injury very similar results are obtained. Results of an identical statistical test indicated that head injuries in the automatic group were significantly more severe than head injuries in the social group (q < .05, P = .0119, H = 13.11) and that head injuries in the automatic group were significantly more severe than extremity injuries in the automatic (q < .05, P = .001, H = 13.11) and social groups (q < .05, P = .0063, H = 13.11).
Discussion
In this study, slightly more than half of individuals who were hospitalised for the treatment of SIB had an injury at intake. In addition, for those with an injury, there was variability in the locations, types and severities of injuries. These results are consistent with previous research on SIB-related injury in this population (Hyman et al. 1990). Directly related to the likelihood of injury, we found that individuals who engaged in a single form of SIB (sharp or blunt) were more likely to have injuries. Although it is logical to assume that a high degree of SIB consistency (in form and target body site) is more likely to produce SIB related-injury, these results provide empirical evidence for this suspicion. Finally, as related to individuals with and without injury, we did not find the rate of SIB in the play condition was generally predictive of injuries. This finding is particularly surprising given that the vast majority of treatments for SIB focus on reducing the rate of this behaviour (e.g. Iwata et al. 1994). However, this finding is limited by the context in which the data were collected, the FA control conditions is meant to reduce individuals’ motivation to engage in SIB, thus future research may wish to design a standard means to assess the rate of behaviour across individuals when investigating SIB-related injuries.
Although our findings are preliminary, we found that the function of SIB predicted the location of injury sites with the most severe injuries across groups. Individuals in the automatic group were significantly more likely to have severe injuries to the head; whereas individuals in the social group tended to have more severe injuries to the torso and extremities. The current findings suggest that the function of SIB may affect how SIB is physically expressed by an individual. Put another way, these results suggest that the reason SIB occurs may influence the injuries subsequently incurred, which implies that the function of SIB may influence the form and location of SIB. For individuals with automatically reinforced SIB, these findings are broadly consistent with previous research, which suggested that preferences for SIB sites could be related to potential sources of automatic reinforcement, such as biological events (Symons & Thompson 1997; Wisely et al. 2002; Breau et al. 2003).
Individuals in the social group were slightly more likely to engage in multiple forms of SIB and produce severe injury to more diverse sites. From a functional perspective, for socially maintained behaviour, the audience provides reinforcement, thus the audience ultimately determines the form of SIB that will contact reinforcement. However, the degree to which SIB occurs, including the form and location of that SIB, should also be determined by the pain that it produces. Research has suggested that some individuals with IDD who engage in SIB have heightened sensory perception to tactile stimulation and do experience pain when engaging in SIB (i.e. there is a ‘cost’; Courtemanche et al. 2012; Symons et al. 2010). Thus, it stands to reason that for socially reinforced SIB, these individuals may be more likely to vary the form and location of SIB matching their performance (SIB) to the reward (the functional reinforcer) while minimising the cost (i.e. the pain). Thus, future research on socially reinforced SIB could be conducted from a matching perspective where co-occurring reinforcement and aversive consequences are present (e.g. Yoshino & Reed 2008).
Additionally, future research is needed to develop a model that more accurately determines risk of injury secondary to SIB in prospective manner, which could be used during clinical care. The current results suggest that, at minimum, this preliminary model might incorporate contextual variables (such as the function of behaviour or current medications), as well as the physics of the act (such as properties of the action and body site being targeted), to forecast the potential risk of injury. Future research using such a model has the potential to inform a more systematic investigation of SIB-related injury production.
Limitations
The findings in the current study should be tempered by a few weaknesses, most obviously the source of the data and limited analysis that could be conducted. Although all of the individuals with injuries engaged in SIB, the injury was produced prior to their admission to the hospital, thus there is no guarantee that any injury was actually produced by SIB. Further, although the clinical care records provided a wealth of information, more detailed descriptions on the properties of SIB and history of engaging in SIB would have led to a richer analysis. Perhaps most importantly, although the data collected were substantial (results of 64 physicals with approximately 100 injury sites and hundreds of FA sessions), given the number of individuals and the number of particular wounds (e.g. low levels of torso wounds), more sophisticated statistical modelling could not be conducted. Thus, the current approach of examining each predictor variable independently may be prone to false positives, and the findings should be considered preliminary. We attempted to mitigate this weakness by using posttests that allowed for FDR; however, more sophisticated analyses related to the variables that predict injury and differences in injury across functional classes of SIB are needed. Finally, studying automatically or socially reinforced SIB as a single functional category may not be appropriate, as doing so ignores major differences in the clinical presentation of different subtypes of automatically and socially reinforced SIB (Iwata et al. 1994; Hagopian et al. 2017).
Conclusion
This study summarises the functions and injuries of 64 individuals who engaged in SIB. Results, although preliminary, indicate differences in injury severity and location of injury sites across groups of individuals with automatically and socially reinforced SIB. These results suggest that the function of SIB affects the physical properties of how SIB is expressed and the nature of SIB-related injuries.
Supplementary Material
Figure S1. The severity of each injury at each injury site for all individuals, separated by group.
Acknowledgements
Manuscript preparation was supported by Grant R01 HD076653 and from the Eunice K. Shriver National Institute of Child Health and Human Development (NICHD). The contents are solely the responsibility of the authors and do not necessarily represent the official views of NICHD. Special thanks to the members of the Nursing Department of the Neurobehavioral Inpatient Unit, without whom this research could not have been conducted. Special thanks to Erica Lozy, who assisted in gathering interobserver agreement data.
Footnotes
Supporting Information
Additional Supporting Information may be found online in the supporting information tab for this article.
In the vast majority of cases, the rate of SIB was measured in the FA; in one individual’s FAs, the latency to the first instance of SIB was measured.
Structural criteria rules available from the first author upon request.
For the individual in the automatic group, SIB was only assessed using latency as the dependent measure, thus rate data were not available. For the individual in the social group, SIB was maintained by social avoidance. We determined that this case was not appropriate for inclusion, as the control condition was likely to occasion behaviour rather than serve as a control.
References
- Beavers GA, Iwata BA & Lerman DC (2013) Thirty years of research on the functional analysis of problem behavior. Journal of Applied Behavior Analysis 46, 1–21. 10.1002/jaba.54. [DOI] [PubMed] [Google Scholar]
- Benjamini Y, Krieger AM & Yekutieli D (2006) Adaptive linear step-up procedures that control the false discovery rate. Biometrika 93, 491–507. 10.1093/biomet/93.3.491. [DOI] [Google Scholar]
- Breau LM, Camfield CS, Symons FJ, Bodfish JW, MacKay A, Finley GA et al. (2003) Relation between pain and self-injurious behavior in nonverbal children with severe cognitive impairments. The Journal of Pediatrics 142, 498–503. 10.1067/mpd.2003.163. [DOI] [PubMed] [Google Scholar]
- Cooper SA, Smiley E, Allan LM, Jackson A, Finlayson J, Mantry D et al. (2009) Adults with intellectual disabilities: prevalence, incidence and remission of self-injurious behaviour, and related factors. Journal of Intellectual Disability Research 53, 200–16. 10.1111/j.1365-2788.2008.01060. [DOI] [PubMed] [Google Scholar]
- Courtemanche A, Schroeder S, Sheldon J, Sherman J & Fowler A (2012) Observing signs of pain in relation to self-injurious behaviour among individuals with intellectual and developmental disabilities. Journal of Intellectual Disability Research 56, 501–15. 10.1111/j.1365-2788.2011.01492.x. [DOI] [PubMed] [Google Scholar]
- Emerson E, Kiernan C, Alborz A, Reeves D, Mason H, Swarbrick R et al. (2001) Predicting the persistence of severe self-injurious behavior. Research in Developmental Disabilities 22, 67–75. 10.1016/S0891-4222(00)00062-7. [DOI] [PubMed] [Google Scholar]
- Goh HL, Iwata BA, Shore BA, DeLeon IG, Lerman DC, Ulrich SM et al. (1995) An analysis of the reinforcing properties of hand mouthing. Journal of Applied Behavior Analysis 28, 269–83. 10.1901/jaba.1995.28-269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagopian LP, Fisher WW, Thompson RH, Owen-DeSchryver J, Iwata BA & Wacker DP (1997) Toward the development of structured criteria for interpretation of functional analysis data. Journal of Applied Behavior Analysis 30, 313–26. 10.1901/jaba.1997.30-313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagopian LP, Rooker GW, Jessel J & DeLeon IG (2013) Initial functional analysis outcomes and modifications in pursuit of differentiation: a summary of 176 inpatient cases. Journal of Applied Behavior Analysis 46, 88–100. 10.1002/jaba.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagopian LP, Rooker GW, Zarcone JR, Bonner AC & Arevalo AR (2017) Further analysis of subtypes of automatically reinforced SIB: a replication and quantitative analysis of published datasets. Journal of Applied Behavior Analysis 50, 48–66. 10.1002/jaba.368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall SS, Hustyi KM, Chui C & Hammond JL (2014) Experimental functional analysis of severe skin-picking behavior in Prader–Willi syndrome. Research in Developmental Disabilities 35, 2284–92. 10.1016/j.ridd.2014.05.025. [DOI] [PubMed] [Google Scholar]
- Herzinger CV & Campbell JM (2007) Comparing functional assessment methodologies: a quantitative synthesis. Journal of Autism and Developmental Disorders 37, 1430–45. 10.1007/s10803-006-0219-6. [DOI] [PubMed] [Google Scholar]
- Hyman SL, Fisher W, Mercugliano M & Cataldo MF (1990) Children with self-injurious behavior. Pediatrics 85, 437–41. Accessed at: http://pediatrics.aappublications.org/content/85/3/437. [PubMed] [Google Scholar]
- Iwata BA, Dorsey MF, Slifer KJ, Bauman KE & Richman GS (1982) Toward a functional analysis of self-injury. Analysis and Intervention in Developmental Disabilities 2, 3–20. 10.1016/0270-4684(82)90003-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iwata BA, Pace GM, Dorsey MF, Zarcone JR, Vollmer TR, Smith RG et al. (1994) The functions of self-injurious behavior: an experimental-epidemiological analysis. Journal of Applied Behavior Analysis 27, 215–40. 10.1901/jaba.1994.27-215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iwata BA, Pace GM, Kissel RC, Nau PA & Farber JM (1990) The Self-Injury Trauma (SIT) scale: a method for quantifying surface tissue damage caused by self-injurious behavior. Journal of Applied Behavior Analysis 23, 99–110. 10.1901/jaba.1990.23-99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kahng S, Hausman NL, Fisher AB, Donaldson JM, Cox JR, Lugo M et al. (2015) The safety of functional analyses of self-injurious behavior. Journal of Applied Behavior Analysis 48, 107–14. 10.1002/jaba.168. [DOI] [PubMed] [Google Scholar]
- Kennedy CH & Thompson T (2000) Health conditions contributing to problem behavior among people with mental retardation and developmental disabilities In Wehmeyer M & Patten J (Eds.), Mental retardation in the 21st century (pp. 211–31). Austin, TX: ProEd. [Google Scholar]
- Koo TK & Li MY (2016) A guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine 15, 155–63. 10.1016/j.jcm.2016.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roane HS, Fisher WW, Kelley ME, Mevers JL & Bouxsein KJ (2013) Using modified visual-inspection criteria to interpret functional analysis outcomes. Journal of Applied Behavior Analysis 46, 130–46. 10.1002/jaba.13. [DOI] [PubMed] [Google Scholar]
- Soke GN, Rosenberg SA, Hamman RF, Fingerlin T, Robinson C, Carpenter L et al. (2016) Brief report: prevalence of self-injurious behaviors among children with autism spectrum disorder – a population-based study. Journal of Autism and Developmental Disorders 46, 3607–14. 10.1007/s10803-016-2879-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Symons FJ, Harper V, Shinde SK, Clary J & Bodfish JW (2010) Evaluating a sham-controlled sensory-testing protocol for nonverbal adults with neurodevelopmental disorders: self-injury and gender effects. The Journal of Pain 11, 773–81. 10.1016/j.jpain.2009.11.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Symons FJ & Thompson T (1997) Self-injurious behaviour and body site preference. Journal of Intellectual Disability Research 41, 456–68. 10.1111/j.1365-2788.1997.tb00737.x. [DOI] [PubMed] [Google Scholar]
- Thompson T, Symons F, Delaney D & England C (1995) Self-injurious behavior as endogenous neurochemical self-administration. Mental Retardation and Developmental Disabilities Research Reviews 1, 137–48. 10.1002/mrdd.1410010210 [DOI] [Google Scholar]
- Wisely J, Hare DJ & Fernandez-Ford L (2002) A study of the topography and nature of self-injurious behaviour in people with learning disabilities. Journal of Learning Disabilities 6, 61–71. 10.1177/146900470200600105. [DOI] [Google Scholar]
- Yoshino T, & Reed P (2008). Effect of tone-punishment on choice behaviour under a closed economy. European Journal of Behavior Analysis, 9, 43–52. Accessed at: http://www.tandfonline.com/doi/abs/10.1080/15021149.2008.11434294 Accepted 14 June 2018 [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. The severity of each injury at each injury site for all individuals, separated by group.