
Fig. 1.
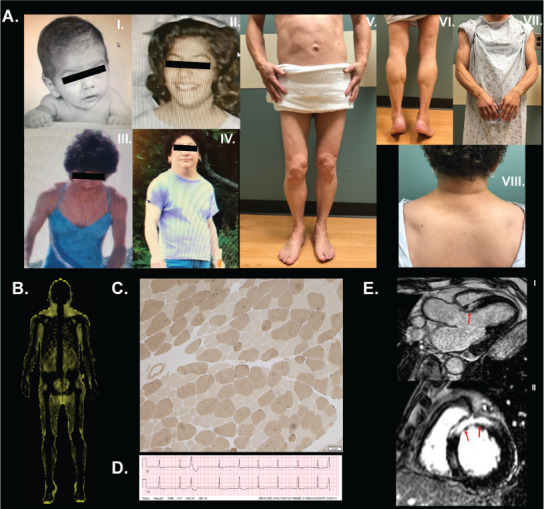
A, Photographs of patient 1 at various ages: (I) a few months old, (II) a teenager, (III) 25 years old, and (IV) 48 years old. We obtained the patient's pictures to demonstrate her current state in October of 2018 with her permission. Close-up pictures of (V) anterior view of the trunk and legs, (VI) back of the legs, (VII) arms, and (VIII) back of the neck. B, “Fat shadow” obtained from dual energy X-ray absorptiometry scan showing fat distribution consistent with generalized fat loss but with some preservation around the neck. Total fat percentage was reported as 22%, the trunk-to-total fat mass ratio was 0.61, and legs-to-total fat mass ratio was 0.24. C, Deltoid muscle biopsy studied with ATPase assay at pH 9.4 with remarkable fiber size disproportion where the type 1 fibers were 45% smaller than the type 2 fibers. Fiber size disproportion (FSD) is an important feature of the Emery-Dreifuss muscular dystrophy (EDMD) pathology and it was remarkably high in our first patient (Fig. 1). Fresh frozen tissue studied for abnormal lack of emerin protein expression by immunohistochemical staining would have been helpful to support the diagnosis of the x-linked form of EDMD caused by STA gene mutation on chromosome Xq28. Most LMNA gene mutations show no alteration in the lamin A/C protein and cannot be detected by immunohistochemical staining. FSD (formerly a subset of congenital fiber type disproportion) is a spectacular feature of a number of muscle abnormalities. The differential diagnosis of muscle diseases that cause FSD includes specific muscular diseases, polymyositis, mitochondrial myopathy, Pompe disease, mutations in the insulin receptor gene, congenital hypothyroidism, phosphofructokinase and carnitine palmitoyltransferase deficiency, and at least 5 congenital myopathies. In this case, the patient's age and presentation decrease this differential. Another important pathologic feature of this case is an ongoing non-inflammatory myopathy, revealed by regenerating muscle fibers. This and steadily elevated creatine kinase levels in this patient's blood suggest a muscular dystrophy. Specific diseases that cause FSD are Becker (more often than Duchenne) muscular dystrohy, myotonic dystrophy, rigid-spine syndrome, and EDMD. Other causes of FSD include certain central nervous system and peripheral nervous system diseases, skeletal disorders, and rare syndromes that do not pertain to this case. D, Electrocardiogram demonstrating first degree atrioventricular block, premature ventricular contractions, and nonspecific ST abnormalities. E, Cardiovascular magnetic resonance images demonstrating extensive late gadolinium enhancement involving the interventricular septum (arrows) consistent with myocardial fibrosis along the (I) apical long axis view and (II) short axis view.