
Fig. 2A-M.
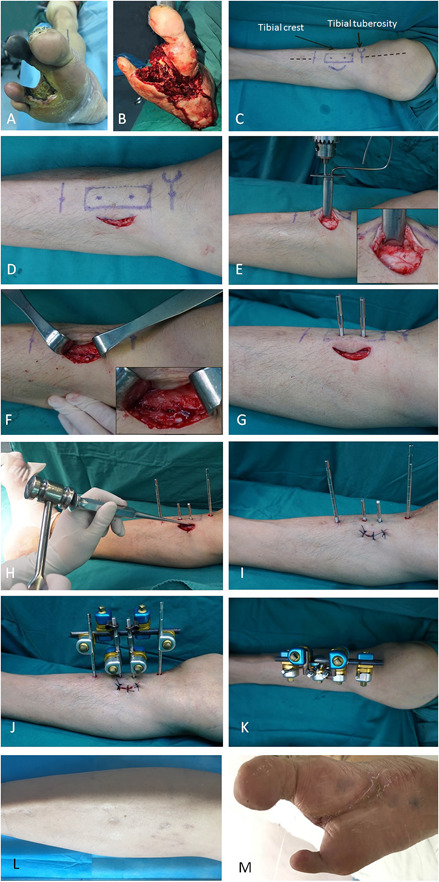
This figure shows the tibial cortex transverse distraction procedure. (A-C) The surgery was performed on the upper 1/3 of the ipsilateral tibia of a foot with a diabetic foot ulcer. (C) The positions of incision, corticotomy, and nailing are shown with markings as part of preoperative planning. (D) A 4-cm medially curved incision was made 1 cm from the tibial crest and 2 cm distal to the tibial tubercle. (E) The soft tissue was retracted with blunt dissection and the periosteum was exposed, which was not removed from the cortex. Corticotomy was performed by drilling multiple holes in a rectangle (1.5 cm × 5.0 cm) in the cortex. (F) Drilling was limited to the ipsilateral cortex, avoiding penetration beyond the depth of the cortex. (G) After osteotomy, two 3-mm drill holes were made in the osteotomized cortex (not extending to the contralateral cortex) followed by the insertion of two pins for distraction. Then, two 4-mm nailing holes extending to the contralateral cortex were made, followed by the insertion of two pins to stabilize the external frame (see Fig. 1, Supplemental Digital Content 7, http://links.lww.com/CORR/A275). (H) The holes were connected using an osteotome to separate the cortex from the tibial shaft. (I) The incision was closed in layers with proper sutures. (J-K) The pins were attached to the fixator frame, which had two screws for distraction. Aggressive débridement was performed to remove nonviable tissues surrounding the ulcer, and minor amputation was performed if necessary. (L-M) The distraction maintained for 4 weeks and then the external fixator was removed. The incision would heal with the ulcer healed gradually.