
Fig. 1.
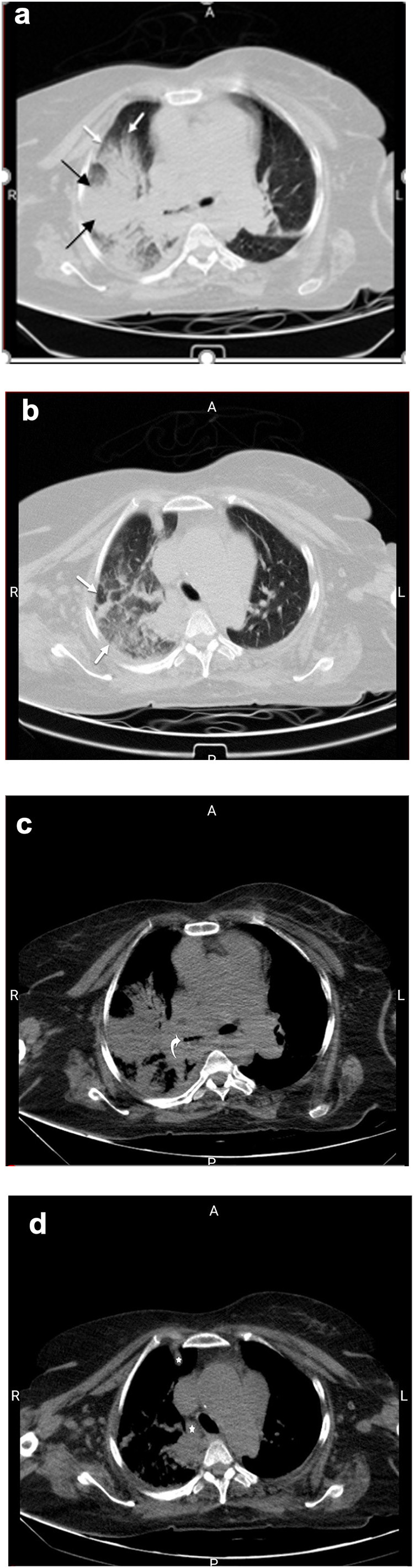
COVID-19 in lung cancer. A fifty-year-old patient with history of lung cancer presented with new-onset fever. Axial images of chest CT reveal lobulated right para-hilar mass (a; black arrows), resulting in post-obstructive collapse and consolidation, consistent with the patient's known lung cancer. Associated ground-glass opacity involving the right upper lung (a, b; white arrows) is also noted, concerning for superimposed atypical infection, such as COVID-19, a diagnosis which was subsequently confirmed with RT-PCR. The narrowing of right main bronchus (c; curved arrow) is also observed. Furthermore, soft tissue window images of the chest reveal prominent right para-tracheal and internal mammary lymphadenopathy (d;☆), which can be metastatic in etiology or reactive to concomitant infectious/inflammatory process.