
Figure 3.
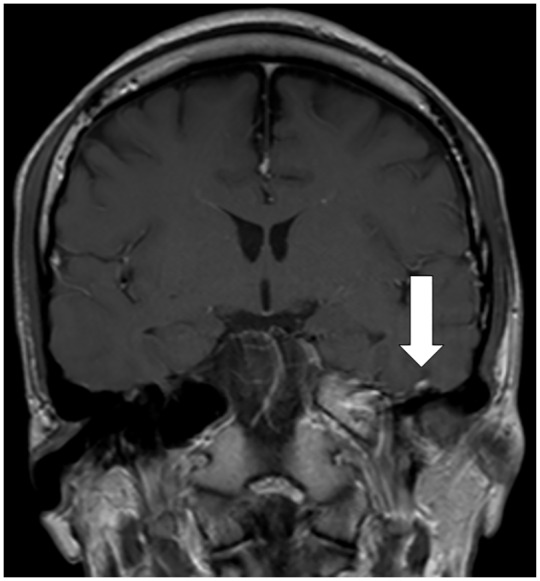
Imaging evaluation of a left facial palsy patient with concomitant COVID-19.
A 27-year-old man was admitted to the isolation ward of a tertiary centre on March 16, 2020, presenting with myalgia, cough, fever and left-sided headache for 4 days. He had just returned from Spain the day before admission. On examination his lungs were clear and neurological examination was unremarkable. Reverse-transcription polymerase-chain-reaction (PCR) performed on the nasopharyngeal swab was positive for SARS-CoV-2. On day 3 of hospitalization, he developed left retro-auricular pain, dysgeusia and left facial weakness. Neurological examination showed a left facial nerve palsy. There was no associated neck stiffness, vesicles in the outer ear, or parotid swelling. Cerebrospinal fluid (CSF) studies showed no cells, and protein and glucose levels were normal. CSF PCR was negative for herpes simplex virus, varicella zoster virus and SARS-CoV-2. His magnetic resonance imaging of the brain showed contrast enhancement of the left facial nerve (Figure). He was treated with lopinavir/ritonavir for reducing SARS-CoV-2 viral replication. He received a 1-week course of prednisolone and valacyclovir for treatment of facial palsy. Upon review 1 week later, his headache had resolved, and improvement was noted in facial weakness.