
Fig. 1.
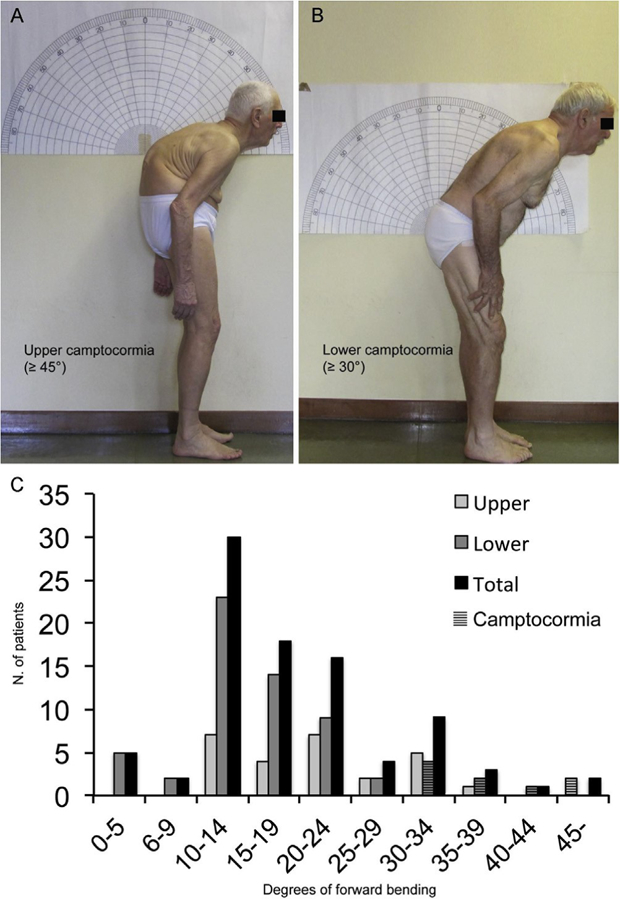
Two example of upper (A) and lower camptocormia (B) according to the definitions reached by full consensus by the panel of experts. Upper and lower camptocormia was measured according to the clinical method used by Furusawa et al. using C7, fulcrum of trunk deviation and the vertical line for the upper camptocormia and C7, sacrum and the vertical line for lower camptocormia [19]. This goniometric modality to quantify postural deformities was chosen due to the relatively easy way to quantify trunk angles during a routine visit and its ability to distinguish two spinal regions (thoracic and lumbar/sacral) which contribute differently to spinal motion [24]. The lumbar/sacral region was considered as a single functional unit because a strict relationship between the pelvic tilt and lumbar lordosis exists during standing posture. Indeed, increasing of the degrees of anterior pelvic tilt increases the angle of lumbar lordosis, and vice versa [25]. Panel C shows the angle distribution of patients with FTB and camptocormia.