

Abstract
Living mindfully helps one gain a deeper understanding into realities of life. It enables people to witness suffering, desire, attachments, and impermanence without any fear, anxiety, anger, or despair. This is considered the hallmark of true psychological insight. As a skill, mindfulness can be inculcated by anyone. Mindfulness helps in attending, getting aware and understanding experiences in a compassion and open-minded way. Research suggests that applying mindfulness in daily life has been known to tame our emotional mind and enabled people to perceive things “as they are” without ascribing expectations, judgments, cynicism, or apprehensions to them. This review unravels the therapeutic power of mindfulness meditation in the context of infertility distress. It serves to integrate the evidence on the effectiveness of mindfulness-based psychological interventions to improve the emotional well-being and biological outcomes in Infertility.
KEYWORDS: Counseling, emotional distress, India, infertility, mindfulness, psychotherapy, review
INTRODUCTION
Infertility is not only a medical condition.[1] It has psychosocial facets as well. These have been extensively elaborately in the existing literature.[1] Researchers over the past few decades have also devised several modules of psychotherapies in order to tackle the emotional and relational distress of patients undergoing fertility treatments The clinical usefulness of mindfulness-based interventions (MBIs) is high, and they are becoming increasingly popular. This form of psychotherapy has extensive applicability for those coping with emotional distress in a range of medical and psychiatric conditions.[2,3,4,5,6,7,8,9,10] Individuals cope with infertility and with the demands of medically assisted reproductive treatments, i.e., intrauterine insemination (IUI), in vitro fertilization (IVF), intracytoplasmic sperm injection, and gamete intra fallopian transfer (GIFT)[11] have also acknowledged the benefits of MBIs.
This paper presents an overview of the original philosophy behind mindfulness, mindfulness in psychotherapy, challenges of coping with infertility, and how MBIs may be applied in this context.
The original philosophy behind mindfulness
Mindfulness has been described in psychology as (a) a state of being, (b) a dispositional (personality) trait or quality, (c) a type of practice, and (d) a classification of therapeutic intervention.[12] Accordingly, one of the earliest definitions of mindfulness in psychotherapy explained it as “the process of paying attention on purpose, in the present moment, nonjudgmentally to allow the unfolding of the moment by moment experiences”.[13] Others have defined mindfulness in psychology as a “multi-component construct, including observing, describing, accepting whatever one is experiencing without judgment and acting with awareness.”[14]
This term was introduced about a century ago by the translator Rhys David when working on Pali texts. “Mindfulness” is rooted in Buddhism in which it is described as one of the essential qualities required to attain enlightenment. To understand mindfulness, it is essential to gain an insight into the philosophy from which it originated. Buddhists believe that there are three pivotal characteristics of human existence. These are suffering, impermanence, and illusion of a unique self. Suffering comes from the ups and downs of life. Experiences such as economic instability, sickness, sadness, loss, isolation, stagnation, uncertainty, aging, or general dissatisfaction are commonly associated with human suffering. It comes from the fear of change and a nonacceptance of the fact that nothing remains the way it is. Adaptation to the changing life demands is a constant process. In Buddhism, it is also believed that the life of any human being revolves around four noble truths. The heart of these truths is that life firstly and foremostly incorporates suffering in some form or the other. This suffering as described above emerges from a desire for wish-fulfillment, betterment, and to accomplish the “idealized self.” All humans are caught in this cycle of desire and suffering. This cycle of self-fulfillment is never-ending as when one desire is met; people tend to take a step further and move to the other. Hence, we are constantly moving and directing our minds and bodies towards an end in life where we wish or see ourselves “to be someone else, have a little more, and to be a bit better.” While planning for all these things, we move away from what we are in, i.e., our present life, its essence, its purpose, its beauty, and its properties. The fourth noble truth is that we can alter and put an end to this cycle of desire and pain. Instead of operating in “the doing mode in which one is driven by desires and goal-fulfillment, if we step back and choose to “pause, acknowledge, decenter, and reperceive certain desires and attachment bonds, the suffering associated with these shall gradually reduce.” Hence, the last noble truth shows one the pathway to end human suffering. This may be related to any human desire. Buddha went on to elaborate that following the noble eightfold path ends suffering. The path speaks of adopting “the middle way in life” by being connected to what “one is in the present,” and “deeds of day to day living.” It also involves empowering the mind by “right understanding, right intent, right speech, right livelihood, right effort, right mindfulness, and right concentration.” Mindfulness practice or meditation is an essential ingredient of “right awareness.” It is the foundation of the mental discipline necessary to achieve the “right concentration, understanding, and thought” that makeup wisdom and insight.
Mindfulness in psychotherapy: A general overview
In the process of unraveling the therapeutic power of mindfulness meditation (MM) and integrating it with conventional psychotherapy, behavioral scientists have developed numerous MBIs. The first of the MBIs was mindfulness-based stress reduction.[15] The program is described as a group-based module consisting of 8 weekly sessions. It emphasizes on being aware of the sensations within the body and then expanding this to regulate emotions and thoughts. Mindfulness-based stress reduction (MBSR) aims to help people develop an ongoing practice to combat emotional distress associated with physical pain. Several other interventions have been designed based on the original model of mindfulness and have been proved as efficacious. More recently, the mindfulness-based cognitive therapy module (MBCT) was developed which is also an 8 weeks module to reduce relapse and recurrence of depression.[16] Other modules of MBIs include “acceptance and commitment therapy, mindfulness-based relationship enhancement (MBRE), and comprehensive mind and body interventions.” MBIs have also been tried out in infertility, and its efficacy has been established in some of the recent studies.[17,18,19,20,21]
Challenges of coping with infertility and how mindfulness-based interventions may be applied in this context
Infertility, unlike any other medical condition, is described as a “low control situation.”[1] Reviews[22] have pointed out that emotional adjustment in couples with infertility is complex as couples have to deal with the following issues, namely:
Stress of infertility diagnosis
Infertility associated identity crisis
Dealing with the ongoing infertility treatment
High possibility of unsuccessful treatment cycles
Choosing treatment options (like donor programs, adoption, etc.)
Uncertainty of outcomes of consecutive cycles (nonresponse, abandonment, failure)
Unwanted effects (repeated cycles of treatments, multiple gestations, going in for fetal reductions, high rates of miscarriages, limited live birth rates, and other obstetric risks).
Coping problems are common among infertile men and women.[1] Emotional well-being and maladaptive coping are reciprocally related to each other. It is known to determine the fate of pregnancy following treatment via the psychoneuroimmunological pathway.[23] A pure problem-based coping or emotional-based coping is unlikely to benefit the childless marital partners in the long run.[1,24] Reviews suggest that meaning-based coping mediated by MBIs is superior to other ways of dealing with chronic stress of infertility.[11] Furthermore, increasing compassionate acceptance, as well as cognitive decentering from distressing thoughts and feelings, seems to help patients in entangling with infertility distress. Mindfulness as a coping skill enables change in the way one relates to stressors, the associated thoughts, and emotions rather than changing or altering the stress itself. It transforms the perception of self, consciousness, reality, and creates a change in perspectives of “self as content (e.g., I am infertile)” to “self as a context (e.g., I am a person experiencing conception problems).”[25] It allows deliberate exposure, compassionate acceptance as well as the extinction of fears and behavioral avoidance associated with fertility-related stimuli.[16,17,18,19,20,21] The mechanism of change caused by mindfulness-based therapy is twofold. First, mindfulness training leads to stabilization in cognitive capacities, overactive autonomic arousal, and emotional regulation. It helps in breaking out from the vicious cycles of negative thinking in infertility. Second, mindfulness practice involves disease-specific coping with infertility stressors.[26]
Systematic reviews go on to claim that the overall effect size of psychotherapy in couples or individuals with infertility is reported to be higher for MBIs than other varieties of therapies.[11] Recent studies also reveal that the acceptance of MBIs in infertility is fairly high and dropouts are usually low.[27] Research evidence has acclaimed that MBIs are more efficacious than traditional cognitive therapy, behavior therapy, or cognitive-behavior therapy (CBT) in infertility as it focuses on a wider spectrum of psychological problems such as interpersonal, marital, existential, and sociooccupational difficulties.[11] Several others opine that MBIs are superior to the conventional cognitive behavioral therapy, as it trains the participants in nonspecific factors such a higher self-attunement, acceptance, compassion, empathy, openness, and nonstriving, leading to a higher cognitive and behavioral flexibility while responding to stressful events.[28]
Components of mindfulness-based interventions in infertility
The basic premise of treatment (MBIs) is the understanding of the “nature of one's desire and suffering related to the nonfulfillment of this desire.” The philosophy behind MBIs is to develop an insight into the process of emotional distress in infertility. Distress often starts with its diagnosis.[1] It builds up with time when couples are trying very hard to resolve it. Many a times, despite their best efforts, they are unable to meet their expectations.[1] This very often traps them in recurrent or persistent cycles of ruminations, sadness, worries, fear or avoidance, and pushes their minds beyond the limits of “normal emotional response to infertility.” In their desire to overcome childlessness, infertile couples often move away from their usual activities, work, and interpersonal bonds and are unable to cherish their lives and marital relations for what they are. The latter may result in clinical levels of depression and anxiety in men and women.[1] Research suggests that no matter how painful it may appear, intentionally attending to present moment experiences with mindful attitudes such as curiosity, openness, compassion, nonstriving, and nonjudgmental awareness leads to a significant shift in perspective, termed as “reperceiving and value clarification.”[6] Reperceiving builds the self-regulation and self-management capacity of a person.[29] Accordingly, mindfulness coping involves training the mind in purposeful “intention,” “attention,” and “awareness,” and these are the fundamental components of MBIs.[6] Researchers have proposed the following criteria to ascertain whether a person is appropriate and is likely to benefit from MBIs.
Patient suitability for MBIs: It is suitable for people with emotional distress related to any medical condition/type of infertility. Before taking MBIs, participants must understand that it is not a “panacea.” Clients should have the psychological endurance to undergo the intensive 8 weeks process, as it may not be a blissful experience. Such interventions are rather an invitation to explore (one's mind, senses, body, emotions, and thoughts) and a personal journey to understanding self and others[30]
Timing, location, and format of MBIs: In infertility, couples undertake MBIs during their active IUI/IVF or in “waiting periods” of these treatments. Most studies conducted on MBIs in infertility mention that therapy is delivered in group format consisting of women or couples diagnosed with various types of fertility disorders[1,11,15,16,17,18,19,20,21,22,25,26,27,30,31,32,33,34,35,36,37,38,39,40,41,42]
-
Structure and content of therapy: Most MBIs in infertility are targeted at groups of infertile women/couples.[11,31] They are guided by a comprehensive team consisting of infertility experts, nurses, researchers, psychologists, or social workers trained in MBI (who is the group facilitator). Most of the successful MBI programs in infertility consists of a blend of three or more core components of MBSR/MBCT.[1,11,15,16,17,18,19,20,21,22,25,26,27,31,39,41,42] These involve:
- Awareness and informational provision on fertility disorders and their medical management
- Coping with the psychosocial aspect of infertility and emotionally critical periods
- Life style improvement or fertility enhancement.
Duration of treatments: The MBIs consist of one session per week and their duration may range from 8 to 12 weeks.[16,17,18,19,20,21] Therapy is preceded by a precourse orientation and assessment session to ensure patient suitability and willingness for the entire MBI module.[16,17,18,19,20,21] The module intends to teach mindfulness coping skills, the operation of wise-mind and “being mode” into the daily life process by means of formal as well as informal meditation and self-regulation skill training.[16,17,18,19,20,21] All training rests on the pillars of attitudinal transformation such as openness, allowing nonjudging, awareness, acceptance, and compassion for self and others, kindness, and gentle nonstriving.[16,17,18,19,20,21] Each session starts and ends with some form of formal mindful meditation. Overall, the first half of such programs consists of 4 weeks, with a general emphasis on learning to bring attention to “internal” experience and seeing what happens in this process.[16,17,18,19,20,21] The second half of the program consists of the last 4 weeks. These weeks emphasize on the application of mindfulness to life challenges of daily living, understandings that emerge through new meanings, perceptions of current life situations, and dealing with solvable and insolvable aspects of life problems.[16,17,18,19,20,21] Nowadays, brief MBIs (4–6 sessions) are also found to be useful, particularly in facilitating coping with chronic distress of long-term medical illnesses.[32,33,34,35,36,37,38] In addition, several good-quality studies opine that customized MBIs for infertility, interventions with a limited number of techniques such as eating meditation, body scan, sitting and walking meditation, 3 min breathing space, mountain meditation, and other informal practice are found to be effective in reduce negative effects in low control problem situations like infertility[17,18,19,20,21,22,25,27,39,40,41,42]
Expectations from MBI therapist: Training of MBI practitioners is an important prerequisite to delivery of this therapy. Training in medical and psychological aspects of infertility and its treatment is essential.[43] Extensive guidelines for MBI therapists have been established in the existing literature, and these need to be strictly adhered too for both clinical and research purpose[44]
Compliance and its monitoring in MBIs: MBIs tend to heavily rely on the participant's compliance and adherence to structured home practice, with a minimum of 45 min/day of a formal mindfulness practice, daily life informal practices and recording of observations of experiences.[3,16,45,46] A minimum of 20 min of daily home practice is recommended in brief MBIs.[35,36] The total amount of practice recommended is 45 min × 6 days a week (270 min) for 4–5 months is outlined in the standard MBSR/MBCT interventions.[45,46] Factors such as therapist's competence and client's motivation, expectancies, recall biases, difficulty in comprehension, perceived benefits, attendance in initial therapy sessions, and client effort effects the compliance and outcomes.[44,45,46,47] Monitoring of skills by the therapist is important in terms of total frequency and minutes of practice maintained by clients. Another important agenda here is the resources and guidance provided to the clients to comply to MBIs. Most importantly, clients are provided written materials, audiovisual CDs, audio recordings of coping skills to maintains revision of session content, and home practice of MMs[3,13,15,16]
Computer-aided, internet-based, and smartphone applications of MBIs: The effectiveness of newer well-designed computer-aided, internet-based, and smartphone applications of MBIs[48] is appreciable in reducing depression, stress, anxiety, in normal and clinical population.[4,7,8,9,10,12,48,49,50,51] However, the effectiveness of such formats in infertility has not been very well documented
Booster sessions for MBIs: In the follow-up period, posttherapy, 3–4 reinforcement sessions are recommended.[3,13,15,16] This helps in addressing the participant's hurdles to home practice as well as consolidates their meditation skills as well as therapeutic learning.
Expected outcomes from patients
MBIs led to reduction in emotional distress, pain perception, depression, and anxiety after 3–6 months of continued practice.[52] A study by Williams et al. urges that a home practice of three or more days a week reduces the risk of depressive relapse by 50%.[5] Furthermore, the same amount is suggested to reduction of anxiety symptoms[53] and it is believed that a home practice of <2 days a week is insufficient. Participants with higher in-session engagement spend more in home practice of skills and are thus likely to experiences better outcomes.[54]
Neurocognitive effects of mindfulness meditations
MMs may induce specific, functional, i.e., “state-dependent” changes in brain activity,[55,56] suggesting an increased involvement of attentional control processes during meditation. In line with this interpretation, mindfulness meditators compared to nonmeditators, show superior executive control mechanisms and reduced automated responding[57] and reduction in free-wandering non emotional thoughts, and P3a component of the event-related potential, indicative of reduced evaluative processing.[58] Mindfulness practice reduces the activation of the “default mode of the brain,” which is concerned with searching for problems in one's life, and anticipating solutions for it.[59] Practice of MM increased oscillation over parietooccipital brain areas in the gamma frequency range (35–45 Hz), thus causes an increase in sensory awareness.[57] The MBSR participants show a more pronounced reduction of activity in the medial prefrontal cortex during present-moment as compared with self-related attention and showed higher activity in a network lateralized to the right hemisphere.[60,61] This network comprised the right prefrontal cortex and several viscerosomatic areas. During induction of sadness, the same network was recruited more strongly in MBSR participants than in controls, and improving their ability to balance affective and sensory neural networks, led to reduced vulnerability to dysphoric reactivity.[60,61] Practice of MM is associated with a more “detached observation of the state of events” characterized by reduced emotional reactivity.[62]
Certain structural changes are also observed in the brains of people who practice mindfulness regularly. Greater cortical thickness in the anterior cingulated gyrus, the parahippocampal gyrus, and the anterior insula was furthermore related to reduced pain sensitivity in Zen mindfulness meditators. Furthermore, a reduction of gray matter density in the right basolateral amygdala, which was positively correlated to the stress levels, is also reported.[55,56] One of these studies also demonstrated possible positive effects of MBSR on mood states, cognitive states, and immune system reactivity.[63,64]
Risks of mindfulness-based interventions
Delivery of MBIs by inexperienced practitioners explains poor results obtained from certain investigations.[44]
Harms involved
Effects such as exhaustion, feelings of disorientation, and depersonalization are noted in certain MBSR programs. Appropriate guidance and support by therapist helps in navigating the potentially effects.[65] Other adverse effects include increase in distress or anxiety due to increase in awareness training and inadequate teacher support provided during the initial sessions.[66] Shapiro reports adverse effects in three major domains: (i) intrapersonal (e.g., increased negativity, disorientation, addiction to meditation, boredom, pain), (ii) interpersonal (e.g., family conflicts, more judgmental), and societal effects (e.g., increased alienation), and (iii) discomfort with the real world, ambiguous social reactions to pragmatic mindfulness-based interpretations).[67]
Review question
In the context of the above background, the research questions of the current review are “Is mindfulness training beneficial for distressed individuals with infertility?”
Methods
This is a narrative review informed by a systematic search strategy. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was used to guide our overall approach and writing structure, but not all of the PRISMA items were applicable to our review question.
Search strategy
In January 2019, we systematically searched databases such as SCOPUS, PubMed, and Springerlink using keyword strings of “mindfulness OR mindfulness based therapy OR mindfulness training AND infertility OR women OR men OR couples” to identify relevant studies published in English language since 1990.
Eligibility criteria and study selection
The review chooses to focus on men and women diagnosed with primary or secondary infertility who participated in face to face sessions of MBSR, MBCT, MBRE, or any other modified versions of the latter in which “mindfulness” had been a core component of therapy. The review included studies in which the psychological intervention has been delivered by a well-trained in MBIs, the therapist was a qualified psychiatrist/psychologist/psychiatric or medical social worker and had the experience of working in the field of reproductive medicine/psychology. This review restricts itself to randomized trials or non-randomized controlled trials (RCTs) as well as interventional studies that were quantitative by nature and were conducted in a clinical or a community setting. In case of an RCT/non-RCT (NRCT), the eligible control groups included participants receiving no treatment, waitlist control, or alternative psychological intervention. The reviews excludes studies in which the participants were known to have a severe psychiatric morbidity or who were on treatment for same (Organic Mental Disorders, Schizophrenia, Bipolar Affective Disorders, Substance Dependence Disorder, Personality Disorders, or with any other developmentally disorder). The review also excludes studies in which the principal therapist was either inadequately trained to deliver MBIs or was inexperienced to deal with infertile persons. Qualitative studies, review articles, and conference proceedings were also among the exclusions.
Outcomes
Primary outcomes were assessment of the psychosocial outcomes in between various study groups (pre- and post-MBI) including depression, anxiety, stress, pain, perception, well-being, quality of life (QoL), and interpersonal functioning. Secondary outcomes were the biological outcomes in participants (physiological response to ongoing assisted reproductive technology [ART] cycle, pregnancy, live birth, change in biochemical markers of stress, etc.).
Timing and effect measures
Timing of the outcome assessments were pretherapy and posttherapy.
Data collection process
Two authors independently screened all records by title and abstract. Any discrepancies were resolved by further discussion before proceeding to the full-text screening stage. The authors also reviewed the list of selected articles and reference sections were scanned to identify any studies that may have been missed on the electronic database search. Data items were extracted and tabulated included: author details, year, place of study, study design, sample characteristics, outcome measures used, results, and shortcomings. All authors shared auditing of this information for quality control. Discrepancies were resolved by consensus.
Synthesis of results
After studies were identified, we began synthesizing their information by categorizing the study designs and the various ways that the outcomes of MBIs in infertility have been reported in the literature. Values are generally presented in literature as medians and quartile deviations or means ± standard deviation. These were used to calculate the indices of “clinically significant psychotherapeutic change in scores” from the first to last assessment point as per the Blanchard's formula.[68]
RESULTS
Figure 1 presents a PRISMA-inspired flow chart documenting the outcome at each stage of our implemented search process. We shortlisted a total of 9 studies, out of which 3 were RCTs 6 were NRCTS. The characteristics of these studies have been summarized in Table 1.
Figure 1.
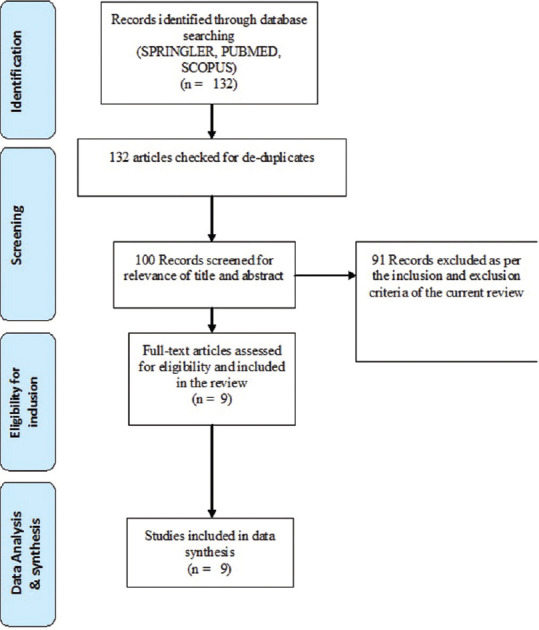
PRISMA for the study
Table 1.
Analysis of Studies on MBIs in infertility
| Author & year | Study Design | Characteristics of Participant | Dose, Nature & Core Content of Psychotherapy | Key Outcomes |
Drawbacks | |
|---|---|---|---|---|---|---|
| Statistically significant improvement in psychological outcomes | Statistically or clinically significant change in Biological outcomes | |||||
| Domar, 1990 | Pre-post design, NRCT | 54 infertile women, their husbands (who were invited for 2 sessions) Some patients in the group were receiving Treatment (IUI or GIFT); others were no longer in ongoing treatment. The majority of the participants had a diagnosis of unexplained infertility. The mean durationof infertility was 3.3 years. |
Nature & Dose :: 10 weekly group based sessions (2 hours duration per session), Program is an Eclectic blend of CBT and mindfulness named as the ‘Mind and Body Program for infertility’. Program was led by a trained Psychologist. | Women : 49%↓Depression/Dejection 44% ↓ Tension/Anxiety, 38% ↓Anger/hostility, 30% ↓Fatigue/Inertia, 31% ↓Bewilderment, 8% ↓ State and trait Anxiety and 9%↓ in Anger expression (as assessed on POMS, STAI) |
34% ↑ in conception rates over a follow up of 6 months. Spontaneous decreases in situational Anxiety related to pregnancy and increases in it related to non-pregnancy. | Uncontrolled preliminary investigation, conducted on a selective sample of infertile women willing to undergo therapy, low power and limited generalizability of results |
| Content & Skills: Introduction to the physiology of stress, the relaxation response, and the relationship between stress and reproductive system, diaphragmatic breathing and mini-relaxation-response exercises, life style modification, cognitive restructuring and affirmations, developing self-empathy and compassion, half-day session, mindfulness practises and attitudes, handling the emotions, anger and forgiveness, all day retreat and review . Peer mentoring: In some sessions peer counsellors (who were diagnosed with infertility and were successful graduates of the course in past) were invited to share their experiences, educate and motivate others with their accomplishments and personal stories. | ||||||
| Sheratt and Lunn, 2013 | Pre-post intervention design, NRCT | 13 women with fertility problems ranging 1 - 4 years . In terms of concurrent treatments, one woman was also undertaking cognitivebehavioural therapy, two women were engaged in IVF and three women were seeing an acupuncturist. | Nature & Dose : : 8 weekly sessions of MBCT (group based) (2 hours duration per session), Program was led by a trained Psychologist. Audio visual materials provided for home practise. | Women Who had attended all of the earlier sessions and maintained a minimum of 30-40 minutes of home practise of 50% of skills (n=10), went on to experience :- 92% ↑in wellbeing 39% ↓ in perceived problems 31% ↑ in daily functioning 70% risk reduction (as assessed on WHO well-being questionnaire and CORE-OM) |
Not assessed | Uncontrolled study with limited sample, low power, non-generalizability of results, follow-up data is incomplete and there is an inappropriateconsideration of concurrent therapies taken by clients. |
| Content & Skills: The first half of the program was developed to train participants to learn to bring themselves back to present moment awareness over and over again and living a daily life with mindful qualities. These included the body scan, an exercise in which participants focus their attention on different parts ofthe body in sequence; mindful movement, in which participants work through a series of directed gentle exercises, keeping their attention focused upon their experience; and sitting meditations, in which participants are directed to focus on their breath, before broadening their attention to sounds and their wider experiencein the room. The second half focussing on applying mindfulness to challenging fertility related situations, experiencing pain, negative emotions or other unpleasant sensations. The aim was to foster the ability to move closer to difficulties and explore them with openness, non-labelling and curiosity. At the end of the programme, participants were helped to think about how they could make mindfulness practice a part of their regular routine in the future. | ||||||
| Psaros, 2014 | Pre-post intervention design, NRCT | 51 Women with any diagnosis of infertility participated. Exclusion criteria included active or untreated major mentalillness that would interfere with study participation (e.g. untreated psychosis or active suicidality), history or currentuse of formal RR-eliciting techniques (including past participationin a mind-body program for infertility), or participationin a donor oocyte in vitro fertilization program. They received standard fertility care during study. |
Nature & Dose : The MBI was a eclectic module, involved a 10-week group program conducted by a trained nurse practitioner . Each session was of 2 hours long. Audio visual materials provided for home practise. | Women Relaxation based skills were practised on average of 15 minutes per day for 5 times per week. 12 months after MBI compliance was 55%. 17% ↑ in perceived social and marital support 43% ↓in depression 28% ↓ perceived stress due to infertility 8% ↓ in pessimism 7% ↑ in optimism (as assessed on MOS, BDI-II, PSS-4, LOTS-R) |
No change detected in Cortisol and AMH as biomarkers from pre-post MBI. At 12-months post-intervention, 51.0% reported conceiving, 23%reported achieving live birth, 22% had an ongoing pregnancy at the time of survey and 6% experienced a pregnancy loss. |
Uncontrolled study, restricted sample, low power, non-generalizability of results, baseline stress being moderate or low in clients which provides a poor rationale for offering them therapy. |
| Content : The program was multidimensional and included daily elicitation of the Relaxation Response using a variety of methods (including breath focus, single-pointed focus, imagery, contemplation, yoga and mindful awareness), the promotion of adaptive cognitive coping and cognitions (e.g. optimism and acceptance), and an assessment of health enhancing behaviours (e.g. individualized recommendations for pre-conception nutrition, exercise and restorative sleep). The weekend session involved husband’s participation to foster a shared experience of the mind-body skills including elicitation of the RR through meditation, partner yoga, mindful walking, humor, social support (for the individual and couple) and education. | ||||||
| Galhardo et al.,2013 | NRCT | 92 women diagnosed with primary infertility 55 participants in MBI group (husbands attend three sessions) and 37 in control group. |
Nature & Dose :The intervention was developed and named as Mindfulness Based Program for Infertility (MBPI) and consisted of 10 weekly sessions, 2 hours each with the sixth session being a full day retreat, administered by a trained Psychologist. Content: The MBPI is intended to develop willingness/acceptance of infertility through a process of contacting the present moment and beingin touch with the unfolding experience in an open and nonjudgmental way. Therapy consisted of training patients using practise and audio-visual tapes for ‘being in the present moment, eating meditation, body scan meditation, three minutes breathing space, sounds and thoughts meditation, inviting a difficulty, being where we already are, leaves in the stream and mountain meditation’ and lifestyle education. Another important skill learned during the MBPI is cognitive defusion or cognitive decentering. Recognizing that our mind tends to create stories about our lives, it is important to help people to become aware of their story as a story instead of a set of‘‘truths’’. |
Women 45%↓ in Depression 10%↓ in Anxiety 22%↓ in Shame 33%↓ in Entrapment 26%↓ in Defeat 12% ↓ in over judgement 2% ↑ in Compassion 20% ↑ in self efficacy to deal with infertility 16%↓ in psychological inflexibility/experiential avoidance. (as assessed on BDI, STAI, OAS, ESS, ES, DS, AAQ, SCSC, SCSJ, ISE) |
Not assessed | Uncontrolled trial, low generalizability of results, Recruitment bias, Participants in both groups were at different stages of their medical treatment and this could have added to a number of confounders. |
| Galhardo et al.,2017 | NRCT | 92 women diagnosed with primary infertility 55 participants in MBI group (husbands attend three sessions) and 37 in control group. Participants in both groups were pursuing infertility medical treatment |
Dose & Content: The dose and content were same as the MBPI (as explained above) and consisted of 10 weekly sessions, 2 hours each with the sixth session being a full day retreat, administered by a trained Psychologist. Audio visual materials provided for home practise. | Women In experimental group experienced an improvement in self efficacy followed by reduction in depression. Inverse was true in parallel controls. Mindfulness coping mediates between self-efficacy and depression among infertile women. (as assessed on BDI, ISE) |
Not assessed | Uncontrolled trial, Participants were allocated to the MBPI condition and to the control group based on geographical criteria, Participants’ recruitment was conducted via the Internet, study conducted on people who were highly motivated for MBI. In addition, the findings clarify one of the mechanismsby which the MBPI exerted its effect, but other processes may have occurred contributing to its efficacy. |
| Li et al, 2016 | NRCT | 58 completed the intervention, and 50 were assigned to a control group. All infertile women registered for their first IVF treatment, did not have mental disorder diagnosis or take psychological treatment in past. | Nature & Dose :The treatment was developed and named as the Mindfulness-Based Intervention for IVF women(-MBII), tailored to match the population . This MBII consists of a six week course, conducted in groups, with one session of 2-2.5 hours duration per week. It was conducted by trained Psychologists. Audio visual materials provided for home practise. Content: This intervention incorporates the following approaches to cultivating mindfulness: (1) mindfulness of thoughts and feelings through breath, thoughts and emotions awareness, and contemplative practices, (2) mindfulness of the body through guided body scan, body awareness meditation and mindful hatha yoga, (3) presentation of psychological concepts that incorporate mindfulness attitudes such as acceptance, letting go, patience and cultivation of an observing self, and (4) waving the mindfulness practices into the daily life, especially during the IVF-treatment, such as doctors’ visit, medical check-up, operation. |
Women 22%↓ in Active avoidance Coping 22%↓ in Passive avoidance Coping 23%↑in Meaning based coping 14% ↑ in mindfulness 22↑in Fertility related quality of Life ( as assessed on SCS, FertiQol, DERS, Ch-FFMQ, COMPI) |
The pregnancy rate was 44% and 26% in the Experimental group and the control group, respectively. | Uncontrolled study, low generalizability of results, lack of a follow uptime point, use of self-report tools, study did not examine the effect of this MBII on physiologic parameters, , single clinic based study. |
| Nery 2018 | RCT | 62 women from the MBP group and 37 from the control group | The MBP intervention was administered to small groups who met for 2 hours weekly during 10 consecutive weeks. The intervention comprised one introductory meeting, eight MBP sessions, and one concluding meeting. The sessions included meditation, relaxation, autogenic training, guided imagery, and biofeedback etc., The control group attended the first and the last meetings but did not attend the MBP sessions. The time interval between allocation and the first group meeting ranged from 1 to 2 weeks. | Women in MBP group vs controls 20% ↓in stress 45% ↓ in depression 19% ↑ in wellbeing Women in Control group No significant change (as assessed on BDI, PGWBI, Lipp’s Stress SymptomsInventory) |
- | Performance bias, lack of blinding, attrition bias is high, participants that perceived a greater benefit of the MBP were more likely to remain in the program leading to overestimation of the benefits of the intervention. |
| Fard, 2018 | RCT | 30 women in MBI and 30 controls undergoing ART | Nature and Dose: The experimental group received MBI in eight group sessions (120 min each) over 8 weeks. The first mindfulness module focused on the basic requirements for mindfulness practice with several basic exercises, such as breathing exercises and a body scan. The second module expanded the first module and consisted of paying attention to develop the ability to flexibly and intentionally switch from one aspect of infertility stress (the need for parenthood) to another (social concerns). The third mindfulness module emphasized the acceptance of unchangeable events (a child-free lifestyle). The participants learned to deal with failures of the ART procedure and living without childbirth. The fourth mindfulness module focused on the realization and nonjudgmental comprehension of the momentum of thoughts, especially about social concerns, marital concerns, and relationship concerns. In the fifth mindfulness module, the participants learned to detach themselves from unwanted thoughts about the fivedomains of infertility stress (the need for parenthood, rejection of a child-free lifestyle, social concerns, marital relationship problems, and sexual concerns) by focusing on the present moment with a nonjudgmental attitude. | Women in MBI group vs controls 22% ↑ in self acceptance 20% ↑ in personal growth 22% ↑ in relationship with others 19% ↑ mastery and autonomy 18% ↑in purpose in life 22% ↑in wellbeing Women in Control group 15% ↑ in self acceptance No significant change on personal growth, relationship with others, mastery, autonomy, purpose in life and wellbeing. (as assessed on -Ryff’s Well-Being Questionnaire) |
- | Small sample size, use of self report measures, recruitment bias, lack of assessment clinical outcomes, lack of blinding, no follow up conducted, lack of assessment of compliance of skills. |
| Patel, et al.,2014-2019, India (Completed trial, results awaited) |
RCT | 36 infertile couples in MBI group and 41 Parallel Controls. All participants were undergoing IUI. | Nature& Dose: The treatment was developed and named as the Modified Mindfulness-Based Cognitive Therapy, and tailored to match the local population and problem being addressed. The intervention consists of one pre-session and 6 sessions of daily therapy with 1.5 hours per session, delivered to the couple. Program is conducted by a Reg. Clinical Psychologist trained in MBIs, infertility and reproductive psychology. Written handouts of sessions, Audio recording of skills done on the patient’s smart phones. Content: Pre-session: Psycho-education and psychological preparation of couples for upcoming IUI+MBCT. Rest of the sessions was based on following content: 1) Distress and automatic pilot mode. Introducing mindful living and therapeutic pillars, 2: Dealing with barriers with integration of formal and informal mindful practises in daily life, 3) Staying in the present with 3 minute breathing space, 4) Accepting limits, letting be/letting go, 5) Thoughts are not facts, 6) Extending mindfulness to the unsolvable problems and using what has been learnt in this module to deal with future moods. |
Results Awaited | Results Awaited | Awaited |
Footnote: NRCT: Nonrandomized Control Trial, RCT: Randomized Control Trial, POMS: Profile of moods states, STAI: State Trait Anxiety Inventory, IUI: intra-uterine insemination with the use of one’s own gametes, IVF: In vitro fertilization with the use of one’s own gametes, GIFT: Gamete intra fallopian transfer, MBCT: Mindfulness based Cognitive therapy, MBI: Mindfulness based intervention, CORE-OM: Clinical outcomes in routine evaluation questionnaire, WHO: World Health Organization, AMH: anti-Mullerian Hormone, MBPI: Mindfulness Based Program for Infertility, BDI : Becks Depression Inventory, OAS: Others as shame scale, ESS: Experience of Shame Scale, ES: Entrapment Scale, DS: Defeat Scale, AAQ: Acceptance and Action Questionnaire, SCSC: Self-Compassion Scale-compassion component, SCSJ: Self-Compassion Scale- self judgment component, ISE: Infertility self efficacy scale, MBII: Mindfulness-Based Intervention for IVF women, FertiQol: Fertility related quality of life questionnaire, DERS: Difficulties in Emotion Regulation Scale, , Ch-FFMQ: The Chinese version of Five Facet Mindfulness Questionnaire, COMPI: The Copenhagen Multi-Centre Psychosocial Infertility, PGWBI: Psychological General Well Being Inventory. * Most of literature on psychological interventions in infertility carries a high risk of bias31. This bias is evident on several domains (sample selection, detection, procedural, assessment and attrition, as well as the evaluation of outcomes and reporting of results). Thus discussion of results in this chapter would largely be carried out in light of evidences gathered from RCTs and NRCTs (with a low risk of bias) that adhere to principles of evidenced based practise and therapy31. This review excludes case studies, case series and non-specific interventions (such as expressive writing interventions, self-help interventions, internet therapy and music therapy) and studies in which MBIs were delivered by untrained mental health practitioners
A review of existing literature on application mindfulness-based interventions in infertility
Table 1 presents a summary of findings derived from various methodologically sound investigations on effectiveness of MBIs in infertility. The main conclusions which emerge from the present body of literature[31,15,16,17,18,19,20,21,22,25,26,27,39,41,42] are as following:
MBI may lead to a significant improvement in psychological parameters: MBIs lead to reduction in anxiety, depression, stress, anger, and improvement in well-being and QoL of infertile women. These benefits may be primarily attributed to increase in attentional capacity, switch off “the false–fear alarm reaction” and avoidance coping, self-insight, and meta-cognitive processing, which allows a decentered engagement with distressing emotions and thought. As pointed out by previous reviews,[6] mindfulness training reduces the emotional reactivity, dysphoria, and evaluative processing and helps in greater switching between the first- and third-person perspectives. It also strengthens the fluid attention of the mind, curiosity, and awareness of here and now states as well as helps one develop an acceptance of these experiences in a kind manner without trying to manipulate them.[6] Mindfulness intends to provide engagement with problems to gain a clarity and capacity for insightful action as it creates a cognitive, emotional, and behavioral flexibility. All these mechanisms enhance the self-efficacy of women coping with infertility.[18,19] Increase in mindfulness attitudes among the women also indicated that they responded in a more kind, compassionate, receptive, and accepting manner toward themselves and others whether things go well or badly. This also improved their moods, social support, and marital relationships.[41] MBIs also lead to decrease in rumination, thought suppression, and other negative thinking styles, that are associated with poorer emotional outcomes. While the benefits of MBIs in infertility are well-acknowledged worldwide, its effectiveness is being evaluated in the Indian subcontinent[69]
MBI also lead to a significant improvement in biological parameters: Research highlights a plausible relationship between relaxation response and fertility. It is known that emotional stress can cause tubal spasm, anovulation, abnormal gamete transport, progestational deficiencies, and hyperprolactinemia and can potentially lead to the luteinized unruptured follicle syndrome.[42,69,70,71],72,73 On the other hand, MBIs are known to improve quality of sleep,[41] regulation of cortisol levels,[74] activities of the hypthalamic pituitary adrenal axis (HPA),[75] as well as immune functions,[76] all of which are known to play an important role in infertility.[41]
A critical overview of the existing literature on application of mindfulness-based interventions in infertility
On major issue in the existing data is the relative lack of randomized controlled trials (leading to low generalizability). The use of optimal designs for MBSR, MBCT, etc., with active comparison groups studying the results across these varieties of MBIs is scarce. There is a lack of studies that compare the distress reducing outcomes obtained from MBIs with other interventions or therapies in the same patient group. Disparity in the various mindfulness-based assessment measures is also evident. There is also a lack of studies with long-term follow-ups and investigations of effects of booster MBIs on mental health outcomes. It remains uncertain whether a specific set of skills are more effective or whether the overall increase in mindfulness as an attitude or skill improves mental health. This point has also been in highlighted in a previous review.[66] Presence of recruitment as well as publication bias in studies is another major problem that has been identified. One of gaps identified also concerns with the establishment of multiple definitions for MBIs. Another point that arises while comparing the effects of MMs and MBIs (acceptance and commitment therapy, MBSR, and MBCT) since there are significant differences between the central philosophy of these.[8] In addition, attrition factors and adverse effects have rarely been a subject of investigation in most mindfulness studies conducted so far. This has also been reflected by others[49,77] as a central limitation in the present database. Moreover, the long-term effects of compliance as well as booster therapy sessions need to be considered in further studies planned in this area. Experts in the field of mindfulness caution against perceiving it as a “panacea”[52] and reveal that risks, harms, and barriers to home practice are seldom assessed and examined in MBIs.[46,47,52]
We identified a few more areas that were untapped by the current database and require detailed research. These include the rationale behind the choice of using a specific MBI, the extent of professional training and experience of the therapist administering MBI, client suitability/characteristics of the “therapy receivers,” evaluation of the outcomes of therapy in different phases of ART, and measurement of the therapeutic outcomes in terms of progress, strengths, and limitations.
Variability in outcomes from one mindfulness-based interventions to the other
We observed that several factors lead to high acceptance and the variability in effects of MBIS from one study to the other. Some of these variables are: the total duration of therapy, its quality, therapist's personality, adherence, competence, expertise, client's willing and motivation, and compliance to module posttherapy. This finding has also been validated from a prior investigation.[78] Experts opine that the variability in compliance is itself an important variable which explains the differential effects derived from MBIs.[13,15,66] The latter point has also been supported by the findings gathered from this study. Lastly, the effects of MBIs in infertile “couples” as well as in infertile “men” is also one of the neglected areas in the past and requires more attention from researchers.
CONCLUSION
Fertility treatments are scientific marvels that began in 1970s. With increasing popularity, these technologies saw their dawn in India as early as it did in other parts of the world.[79] Over the past 50 years, most countries have come up with an evidenced-based committee reports that elaborate on the clear guidelines for “Addressing psychosocial needs in infertility” with respect to each phase of treatment. When one draws a relative comparison between Indian setups and these international developments, it becomes evident that “protecting the QoL and psychological well-being of couples struggling with infertility” remains an overlooked area. MBIs have been known to have “trans-diagnostic effects.” Its benefits are appreciated in reducing distress in a range of clinical conditions.[52,80] Research evidence[15,16,17],18,19,[20,21,22,25,26,27,39,41,42] have acclaimed that MBCT, unlike CBT, is efficacious over wider spectrum of psychological problems such as interpersonal, existential, marital, and sociooccupational difficulties. Furthermore, increasing meaning-based coping, compassion, acceptance skills, as well as cognitive decentering from negative thoughts and feelings seems to help women in disentanglement with infertility stress.[81] MBIs thus lead to reduced psychological distress and enhanced conception rates in infertility. Within the Indian context, there is a dire need for investigations exploring such outcomes and conducting empirical research in this area.[69,81]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Covington SN. Fertility counseling: Clinical guide and Case studies. United Kingdom: Cambridge University Press; 2015. [Google Scholar]
- 2.Hofmann SG, Sawyer AT, Witt AA, Oh D. The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. J Consult Clin Psychol. 2010;78:169–83. doi: 10.1037/a0018555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Teasdale JD, Segal ZV, Williams JM, Ridgeway VA, Soulsby JM, Lau MA. Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. J Consult Clin Psychol. 2000;68:615–23. doi: 10.1037//0022-006x.68.4.615. [DOI] [PubMed] [Google Scholar]
- 4.Baer RA. Mindfulness training as a clinical intervention: A conceptual and empirical review. Clinic Psychol. 2003;10:125–43. [Google Scholar]
- 5.Williams JM, Crane C, Barnhofer T, Brennan K, Duggan DS, Fennell MJ, et al. Mindfulness-based cognitive therapy for preventing relapse in recurrent depression: A randomized dismantling trial. J Consult Clin Psychol. 2014;82:275–86. doi: 10.1037/a0035036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shapiro SL, Carlson LE, Astin JA, Freedman B. Mechanisms of mindfulness. J Clin Psychol. 2006;62:373–86. doi: 10.1002/jclp.20237. [DOI] [PubMed] [Google Scholar]
- 7.Davis DM, Hayes JA. What are the benefits of mindfulness? A practice review of psychotherapy-related research. Psychotherapy (Chic) 2011;48:198–208. doi: 10.1037/a0022062. [DOI] [PubMed] [Google Scholar]
- 8.Chiesa A, Malinowski P. Mindfulness-based approaches: Are they all the same? J Clin Psychol. 2011;67:404–24. doi: 10.1002/jclp.20776. [DOI] [PubMed] [Google Scholar]
- 9.Gard T, Hölzel BK, Sack AT, Hempel H, Lazar SW, Vaitl D, et al. Pain attenuation through mindfulness is associated with decreased cognitive control and increased sensory processing in the brain. Cereb Corte×. 2012;22:2692–702. doi: 10.1093/cercor/bhr352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wang C, Schmid CH, Rones R, Kalish R, Yinh J, Goldenberg DL, et al. A randomized trial of tai chi for fibromyalgia. N Engl J Med. 2010;363:743–54. doi: 10.1056/NEJMoa0912611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Boivin J. A review of psychosocial interventions in infertility. Soc Sci Med. 2003;57:2325–41. doi: 10.1016/s0277-9536(03)00138-2. [DOI] [PubMed] [Google Scholar]
- 12.Vago DR, Silbersweig DA. Self-awareness, self-regulation, and self-transcendence (S-ART): A framework for understanding the neurobiological mechanisms of mindfulness. Front Hum Neurosci. 2012;6:296. doi: 10.3389/fnhum.2012.00296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kabat-Zinn J. Mindfulness-based interventions in context: Past, present, and future. Clinic Psychol. 2003;10:144–56. [Google Scholar]
- 14.Baer RA, Smith GT, Lykins E, Button D, Krietemeyer J, Sauer S, et al. Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment. 2008;15:329–42. doi: 10.1177/1073191107313003. [DOI] [PubMed] [Google Scholar]
- 15.Kabat-Zinn J. Mindfulness-based stress reduction (MBSR) Constr Hum Sci. 2003;8:73. [Google Scholar]
- 16.Segal ZV, Williams M, Teasdale J. Mindfulness-Based Cognitive Therapy for Depression. Newyork: Guilford Publications; 2018. [Google Scholar]
- 17.Sherratt KA, Lunn S. Evaluation of a group programme of mindfulness-based cognitive therapy for women with fertility problems. J Obstet Gynaecol. 2013;33:499–501. doi: 10.3109/01443615.2013.786031. [DOI] [PubMed] [Google Scholar]
- 18.Galhardo A, Cunha M, Pinto-Gouveia J. Mindfulness-based program for infertility: Efficacy study. Fertil Steril. 2013;100:1059–67. doi: 10.1016/j.fertnstert.2013.05.036. [DOI] [PubMed] [Google Scholar]
- 19.Galhardo A, Moura-Ramos M, Cunha M, Pinto-Gouveia J. How does the mindfulness-based program for infertility (MBPI) work in reducing depressive symptoms? Mindfulness. 2018;9:629–35. [Google Scholar]
- 20.Psaros C, Kagan L, Shifren JL, Willett J, Jacquart J, Alert MD, et al. Mind – Body group treatment for women coping with infertility: A pilot study. J Psychosom Obstet Gynecol. 2015;36:75–83. doi: 10.3109/0167482X.2014.989983. [DOI] [PubMed] [Google Scholar]
- 21.Nery SF, Paiva SPC, Vieira ÉL, Barbosa AB, Sant'Anna EM, Casalechi M, et al. Mindfulness-based program for stress reduction in infertile women: Randomized controlled trial. Stress Health. 2019;35:49–58. doi: 10.1002/smi.2839. [DOI] [PubMed] [Google Scholar]
- 22.Bayer SR, Alper MM. Boston IVF Handbook of Infertility: A Practical Guide for Practitioners Who Care for Infertile Couples. London: CRC Press; 2007. [Google Scholar]
- 23.Rao KA. The Infertility Manual. New Delhi: Jaypee Brothers, Medical Publishers Pvt. Limited; 2018. [Google Scholar]
- 24.Schmidt L, Holstein BE, Christensen U, Boivin J. Communication and coping as predictors of fertility problem stress: Cohort study of 816 participants who did not achieve a delivery after 12 months of fertility treatment. Hum Reprod. 2005;20:3248–56. doi: 10.1093/humrep/dei193. [DOI] [PubMed] [Google Scholar]
- 25.Peterson BD, Eifert GH. Using acceptance and commitment therapy to treat infertility stress. Cogn Behav Prac. 2011;18:577–87. [Google Scholar]
- 26.Alsubaie M, Abbott R, Dunn B, Dickens C, Keil TF, Henley W, et al. Mechanisms of action in Mindfulness-Based Cognitive Therapy (MBCT) and mindfulness-based stress reduction (MBSR) in people with physical and/or psychological conditions: A systematic review. Clin Psychol Rev. 2017;55:74–91. doi: 10.1016/j.cpr.2017.04.008. [DOI] [PubMed] [Google Scholar]
- 27.Galhardo A, Cunha M, Pinto-Gouveia J. Acceptability and feasibility of the mindfulness based program for infertility (PBMI) Eur Psychiatry. 2016;33:S647. [Google Scholar]
- 28.Hayes SC. Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behav Ther. 2004;35:639–65. doi: 10.1016/j.beth.2016.11.006. [DOI] [PubMed] [Google Scholar]
- 29.Shapiro SL. The integration of mindfulness and psychology. J Clin Psychol. 2009;65:555–60. doi: 10.1002/jclp.20602. [DOI] [PubMed] [Google Scholar]
- 30.Oxford Mindfulness Centre (OMC) Is Mindfulness Safe? Oxford, United Kingdom: Oxford Mindfulness Centre; 2016. [Last accessed on 2019 Jan]. Available from: http://oxfordmindfulness.org/news/is-mindfulness-safe/ [Google Scholar]
- 31.Frederiksen Y, Farver-Vestergaard I, Skovgård NG, Ingerslev HJ, Zachariae R. Efficacy of psychosocial interventions for psychological and pregnancy outcomes in infertile women and men: A systematic review and meta-analysis. BMJ Open. 2015;5:e006592. doi: 10.1136/bmjopen-2014-006592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Fortney L, Luchterhand C, Zakletskaia L, Zgierska A, Rakel D. Abbreviated mindfulness intervention for job satisfaction, quality of life, and compassion in primary care clinicians: A pilot study. Ann Fam Med. 2013;11:412–20. doi: 10.1370/afm.1511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bergen-Cico D, Possemato K, Cheon S. Examining the efficacy of a brief mindfulness-based stress reduction (Brief MBSR) program on psychological health. J Am Coll Health. 2013;61:348–60. doi: 10.1080/07448481.2013.813853. [DOI] [PubMed] [Google Scholar]
- 34.Demarzo M, Montero-Marin J, Puebla-Guedea M, Navarro-Gil M, Herrera-Mercadal P, Moreno-González S, et al. Efficacy of 8- and 4-session mindfulness-based interventions in a non-clinical population: A controlled study. Front Psychol. 2017;8:1343. doi: 10.3389/fpsyg.2017.01343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Braden BB, Pipe TB, Smith R, Glaspy TK, Deatherage BR, Baxter LC. Brain and behavior changes associated with an abbreviated 4-week mindfulness-based stress reduction course in back pain patients. Brain Behav. 2016;6:e00443. doi: 10.1002/brb3.443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Schroeder DA, Stephens E, Colgan D, Hunsinger M, Rubin D, Christopher MS. A brief mindfulness-based intervention for primary care physicians: A pilot randomized controlled trial. Am J Lifestyle Med. 2018;12:83–91. doi: 10.1177/1559827616629121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Howarth A, Perkins-Porras L, Smith JG, Subramaniam J, Copland C, Hurley M, et al. Pilot study evaluating a brief mindfulness intervention for those with chronic pain: study protocol for a randomized controlled trial. Trials. 2016;17:273. doi: 10.1186/s13063-016-1405-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Reynolds LM, Bissett IP, Porter D, Consedine NS. A brief mindfulness intervention is associated with negative outcomes in a randomised controlled trial among chemotherapy patients. Mindfulness. 2017;8:1291–303. [Google Scholar]
- 39.Li J, Long L, Liu Y, He W, Li M. Effects of a mindfulness-based intervention on fertility quality of life and pregnancy rates among women subjected to first in vitro fertilization treatment. Behav Res Ther. 2016;77:96–104. doi: 10.1016/j.brat.2015.12.010. [DOI] [PubMed] [Google Scholar]
- 40.Chan CH, Chan CL, Ng EH, Ho PC, Chan TH, Lee GL, et al. Incorporating spirituality in psychosocial group intervention for women undergoing in vitro fertilization: A prospective randomized controlled study. Psychol Psychother. 2012;85:356–73. doi: 10.1111/j.2044-8341.2011.02040.x. [DOI] [PubMed] [Google Scholar]
- 41.Fard TR, Kalantarkousheh M, Faramarzi M. Effect of mindfulness-based cognitive infertility stress therapy on psychological well-being of women with infertility. Middle East Fertil Soc J. 2018;23:476–81. [Google Scholar]
- 42.Domar AD, Seibel MM, Benson H. The mind/body program for infertility: A new behavioral treatment approach for women with infertility. Fertil Steril. 1990;53:246–9. doi: 10.1016/s0015-0282(16)53275-0. [DOI] [PubMed] [Google Scholar]
- 43.Indian Council of Medical Research. New Delhi: Ministry of Health and Family Welfare. Govrnment of India; 2010. [Last accessed on 2019 Mar 30]. Ministry of Health and Family Welfare. Govrnment of India. The Assisted Reproductive Technologies (Regulations) Rules. Available from: http://www.icmr.nic.in/guide/ART%20REGULATION%20Draft%20Rules%201.pdf . [Google Scholar]
- 44.Crane RS, Kuyken W, Hastings RP, Rothwell N, Williams JM. Training teachers to deliver mindfulness-based interventions: Learning from the UK experience. Mindfulness (N Y) 2010;1:74–86. doi: 10.1007/s12671-010-0010-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Santorelli SF, Kabat-Zinn J, Blacker M, Meleo-Meyer F, Koerbel L. Mindfulness-Based Stress Reduction (MBSR) Authorized Curriculum Guide. Center for Mindfulness in Medicine, Health Care, and Society (CFM) University of Massachusetts Medical School. 2017 [Google Scholar]
- 46.Lloyd A, White R, Eames C, Crane R. The utility of home-practice in mindfulness-based group interventions: A systematic review. Mindfulness (N Y) 2018;9:673–92. doi: 10.1007/s12671-017-0813-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Dunn C, Hanieh E, Roberts R, Powrie R. Mindful pregnancy and childbirth: Effects of a mindfulness-based intervention on women's psychological distress and well-being in the perinatal period. Arch Womens Ment Health. 2012;15:139–43. doi: 10.1007/s00737-012-0264-4. [DOI] [PubMed] [Google Scholar]
- 48.Fish J, Brimson J, Lynch S. Mindfulness interventions delivered by technology without facilitator involvement: What research exists and what are the clinical outcomes? Mindfulness (N Y) 2016;7:1011–23. doi: 10.1007/s12671-016-0548-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Bohlmeijer E, Prenger R, Taal E, Cuijpers P. The effects of mindfulness-based stress reduction therapy on mental health of adults with a chronic medical disease: A meta-analysis. J Psychosom Res. 2010;68:539–44. doi: 10.1016/j.jpsychores.2009.10.005. [DOI] [PubMed] [Google Scholar]
- 50.Toneatto T, Nguyen L. Does mindfulness meditation improve anxiety and mood symptoms? A review of the controlled research. Can J Psychiatry. 2007;52:260–6. doi: 10.1177/070674370705200409. [DOI] [PubMed] [Google Scholar]
- 51.Grossman P, Niemann L, Schmidt S, Walach H. Mindfulness-based stress reduction and health benefits. A meta-analysis. J Psychosom Res. 2004;57:35–43. doi: 10.1016/S0022-3999(03)00573-7. [DOI] [PubMed] [Google Scholar]
- 52.Hanley A, Warner A, Garland EL. Associations between mindfulness, psychological well-being, and subjective well-being with respect to contemplative practice. J Happiness Stud. 2015;16:1423–36. [Google Scholar]
- 53.Perich T, Manicavasagar V, Mitchell PB, Ball JR. The association between meditation practice and treatment outcome in mindfulness-based cognitive Therapy for bipolar disorder. Behav Res Ther. 2013;51:338–43. doi: 10.1016/j.brat.2013.03.006. [DOI] [PubMed] [Google Scholar]
- 54.Day MA, Thorn BE, Ward LC, Rubin N, Hickman SD, Scogin F, et al. Mindfulness-based cognitive therapy for the treatment of headache pain: A pilot study. Clin J Pain. 2014;30:152–61. doi: 10.1097/AJP.0b013e318287a1dc. [DOI] [PubMed] [Google Scholar]
- 55.Chiesa A, Calati R, Serretti A. Does mindfulness training improve cognitive abilities? A systematic review of neuropsychological findings. Clin Psychol Rev. 2011;31:449–64. doi: 10.1016/j.cpr.2010.11.003. [DOI] [PubMed] [Google Scholar]
- 56.Hölzel BK, Ott U, Gard T, Hempel H, Weygandt M, Morgen K, et al. Investigation of mindfulness meditation practitioners with voxel-based morphometry. Soc Cogn Affect Neurosci. 2008;3:55–61. doi: 10.1093/scan/nsm038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Moore A, Malinowski P. Meditation, mindfulness and cognitive flexibility. Conscious Cogn. 2009;18:176–86. doi: 10.1016/j.concog.2008.12.008. [DOI] [PubMed] [Google Scholar]
- 58.Cahn BR, Polich J. Meditation (Vipassana) and the P3a event-related brain potential. Int J Psychophysiol. 2009;72:51–60. doi: 10.1016/j.ijpsycho.2008.03.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Gusnard DA, Akbudak E, Shulman GL, Raichle ME. Medial prefrontal cortex and self-referential mental activity: Relation to a default mode of brain function. Proc Natl Acad Sci U S A. 2001;98:4259–64. doi: 10.1073/pnas.071043098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Farb NA, Anderson AK, Mayberg H, Bean J, McKeon D, Segal ZV. Minding one's emotions: Mindfulness training alters the neural expression of sadness. Emotion. 2010;10:25–33. doi: 10.1037/a0017151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Farb NA, Segal ZV, Mayberg H, Bean J, McKeon D, Fatima Z, et al. Attending to the present: Mindfulness meditation reveals distinct neural modes of self-reference. Soc Cogn Affect Neurosci. 2007;2:313–22. doi: 10.1093/scan/nsm030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Kalisch R, Wiech K, Critchley HD, Seymour B, O'Doherty JP, Oakley DA, et al. Anxiety reduction through detachment: subjective, physiological, and neural effects. J Cogn Neurosci. 2005;17:874–83. doi: 10.1162/0898929054021184. [DOI] [PubMed] [Google Scholar]
- 63.Davidson RJ, Ekman P, Saron CD, Senulis JA, Friesen WV. Approach-withdrawal and cerebral asymmetry: Emotional expression and brain physiology. I. J Pers Soc Psychol. 1990;58:330–41. [PubMed] [Google Scholar]
- 64.Davidson RJ, Kabat-Zinn J, Schumacher J, Rosenkranz M, Muller D, Santorelli SF, et al. Alterations in brain and immune function produced by mindfulness meditation. Psychosom Med. 2003;65:564–70. doi: 10.1097/01.psy.0000077505.67574.e3. [DOI] [PubMed] [Google Scholar]
- 65.Hanley AW, Abell N, Osborn DS, Roehrig AD, Canto AI. Mind the gaps: Are conclusions about mindfulness entirely conclusive? J Couns Dev. 2016;94:103–3. [Google Scholar]
- 66.Fjorback LO, Arendt M, Ornbøl E, Fink P, Walach H. Mindfulness-based stress reduction and mindfulness-based cognitive therapy: A systematic review of randomized controlled trials. Acta Psychiatr Scand. 2011;124:102–19. doi: 10.1111/j.1600-0447.2011.01704.x. [DOI] [PubMed] [Google Scholar]
- 67.Shapiro DH., Jr Adverse effects of meditation: A preliminary investigation of long-term meditators. Int J Psychosom. 1992;39:62–7. [PubMed] [Google Scholar]
- 68.Blanchard EB, Schwartz SP. Clinically significant changes in behavioral medicine. Behav Assess. 1988;10:171–188. [Google Scholar]
- 69.Patel A. Effectiveness of Modified Mindfulness Based Cognitive Therapy in Distressed Couples with Infertility, Undergoing Intra-Uterine Insemination. 2015. [Last accessed on 2019 Feb 22]. Available from: http://www.ctri.nic.in/Clinicaltrials/pdf_generate.php?trialid=9324&EncHid=and modid=&compid=%27,%279324det%27 .
- 70.Koninckx PR, Brosens IA. Clinical significance of the luteinized unruptured follicle syndrome as a cause of infertility. Eur J Obstet Gynecol Reprod Biol. 1982;13:355–68. doi: 10.1016/0028-2243(82)90071-5. [DOI] [PubMed] [Google Scholar]
- 71.Edelmann RJ, Golombok S. Stress and reproductive failure. J Reproduct Infant Psychol. 1989;7:79–86. [Google Scholar]
- 72.Harrison RF. Stress spikes of hyperprolactinaemia and infertility. Hum Reprod. 1988;3:173–5. doi: 10.1093/oxfordjournals.humrep.a136670. [DOI] [PubMed] [Google Scholar]
- 73.O'Moore MA, Harrison RF. Anxiety and reproductive failure: Experiences from a Dublin fertility clinic. Irish J Psychol. 1991;12:276–85. [Google Scholar]
- 74.Hou WK, Ng SM, Wan JH. Changes in positive affect and mindfulness predict changes in cortisol response and psychiatric symptoms: A latent change score modelling approach. Psychol Health. 2015;30:551–67. doi: 10.1080/08870446.2014.990389. [DOI] [PubMed] [Google Scholar]
- 75.Witek-Janusek L, Albuquerque K, Chroniak KR, Chroniak C, Durazo-Arvizu R, Mathews HL. Effect of mindfulness based stress reduction on immune function, quality of life and coping in women newly diagnosed with early stage breast cancer. Brain Behav Immun. 2008;22:969–81. doi: 10.1016/j.bbi.2008.01.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Carlson LE, Garland SN. Impact of mindfulness-based stress reduction (MBSR) on sleep, mood, stress and fatigue symptoms in cancer outpatients. Int J Behav Med. 2005;12:278–85. doi: 10.1207/s15327558ijbm1204_9. [DOI] [PubMed] [Google Scholar]
- 77.Goyal M, Singh S, Sibinga EM, Gould NF, Rowland-Seymour A, Sharma R, et al. Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Intern Med. 2014;174:357–68. doi: 10.1001/jamainternmed.2013.13018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Dimidjian S, Linehan MM. Mindfulness practice. In: O’Donohue W, Fisher JE, Hayes SC, editors. Empirically Supported Techniques of Cognitive Behavior Therapy: A Step-by-Step Guide for Clinicians. New York: John Wiley; 2003. [Google Scholar]
- 79.Bharadwaj A. Conceptions: Infertility and procreative technologies in India. Oxford: Berghahn Books; 2016. [Google Scholar]
- 80.Carmody J. Evolving conceptions of mindfulness in clinical settings. J Cogn Psychother. 2009;23:270–80. [Google Scholar]
- 81.Patel A, Dinesh N, Sharma PS, Kumar P, Binu VS. Outcomes of structured psychotherapy for emotional adjustment in a childless couple diagnosed with recurrent pregnancy loss: A unique investigation. J Hum Reprod Sci. 2018;11:202–7. doi: 10.4103/jhrs.JHRS_127_17. [DOI] [PMC free article] [PubMed] [Google Scholar]