
FIGURE 4.
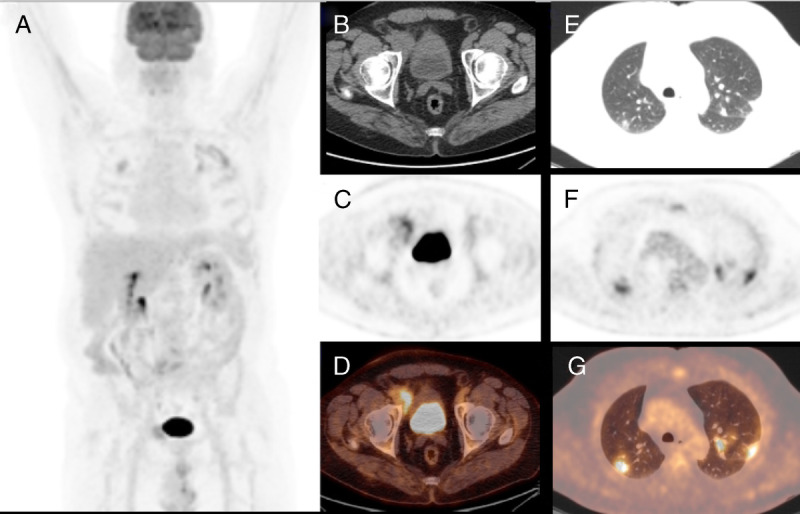
A 62-year-old man affected by follicular lymphoma underwent PET/CT scan for evaluating treatment response after 6 cycles of chemotherapy, and PET/CT showed a partial metabolic response with persistence of increased FDG uptake to an inguinal node (A–D) and the appearance of several bilateral lung consolidative and FDG-avid nodular areas, especially in the superior lobes with SUVmax of 9 (E–G). Being the pattern atypical for COVID-19, the patient started new chemotherapy regimen, but after the early onset of cough and dyspnea, RT-PCR test was done with positive finding for COVID-19. Chest radiographs and CT is the preferred examinations for screening, diagnosis, and monitoring of COVID-19 pneumonia.1–3 In this setting, the role of 18F-FDG PET/CT is still unclear with only few cases present.4–10 18F-FDG PET/CT is a noninvasive tool with a significant role in evaluating several phlogistic and infectious pulmonary diseases, such as sarcoidosis and tuberculosis.11 However, usually lesions presenting as GGOs are unlikely to have FDG uptake.12 In agreement with previous articles,6–8 our patients were characterized by the presence of bilateral peripheral consolidative areas and/or GGOs. All had increased FDG uptake higher than blood pool activity. COVID-19 do not seem to be associated with lymph node involvement; however, Qin et al6 reported an increased nodal FDG uptake in 3 of 4 cases. Of course 18F-FDG PET/CT is not routinely recommended for pulmonary lung inflammatory diseases and not indicated in an emergency setting, but our findings underline that COVID-19 pneumonia are characterized by high 18F-FDG uptake in most cases despite GGOs appearance.