

Summary
Background
Chilblains (‘COVID toes’) are being seen with increasing frequency in children and young adults during the COVID‐19 pandemic. Detailed histopathological descriptions of COVID‐19 chilblains have not been reported, and causality of SARS‐CoV‐2 has not yet been established.
Objectives
To describe the histopathological features of COVID‐19 chilblains and to explore the presence of SARS‐CoV‐2 in the tissue.
Methods
We examined skin biopsies from seven paediatric patients presenting with chilblains during the COVID‐19 pandemic. Immunohistochemistry for SARS‐CoV‐2 was performed in all cases and electron microscopy in one.
Results
Histopathology showed variable degrees of lymphocytic vasculitis ranging from endothelial swelling and endotheliitis to fibrinoid necrosis and thrombosis. Purpura, superficial and deep perivascular lymphocytic inflammation with perieccrine accentuation, oedema, and mild vacuolar interface damage were also seen. SARS‐CoV‐2 immunohistochemistry was positive in endothelial cells and epithelial cells of eccrine glands. Coronavirus particles were found in the cytoplasm of endothelial cells on electron microscopy.
Conclusions
Although the clinical and histopathological features were similar to other forms of chilblains, the presence of viral particles in the endothelium and the histological evidence of vascular damage support a causal relation of the lesions with SARS‐CoV‐2. Endothelial damage induced by the virus could be the key mechanism in the pathogenesis of COVID‐19 chilblains and perhaps also in a group of patients severely affected by COVID‐19 presenting with features of microangiopathic damage.
What is already known about this topic?
Despite the high number of cases of chilblains seen during the COVID‐19 pandemic, a definite causative role for SARS‐CoV‐2 has not yet been proven.
Different pathogenetic hypotheses have been proposed, including coagulation anomalies, interferon release and external factors.
What does this study add?
The demonstration of SARS‐CoV‐2 in endothelial cells of skin biopsies by immunohistochemistry and electron microscopy confirms that these lesions are part of the spectrum of COVID‐19.
Virus‐induced vascular damage and secondary ischaemia could explain the pathophysiology of COVID‐19 chilblains.
Our findings support the hypothesis that widespread endothelial infection by SARS‐CoV‐2 could have a pathogenetic role in the severe forms of COVID‐19.
Linked Comment: Wetter. Br J Dermatol 2020; 183:611.
Acral purpuric lesions identical to chilblains are being seen with an exceedingly high frequency in children and young adults during the coronavirus disease 2019 (COVID‐19) pandemic worldwide.1–3 They have been the subject of numerous mentions in the nonspecialized media, usually under the designation ‘COVID toes’.4 Most patients have been negative for severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) when tested by polymerase chain reaction (PCR) of nasopharyngeal and oropharyngeal swabs, and < 50% have a history of exposure to positive household contacts or previous history of mild upper respiratory or gastrointestinal symptoms.1
Despite the high number of cases, a definite causative role for SARS‐CoV‐2 has not been proven. Several pathogenetic hypotheses have been proposed, including coagulation anomalies, interferon release and external factors.5, 6 On the other hand, the histopathological features of COVID‐19‐related chilblains and the presence of SARS‐CoV‐2 in the lesions have not been addressed.
We present the histopathological, immunohistochemical and ultrastructural features of seven children with chilblains presenting shortly after the peak of the COVID‐19 outbreak in Madrid, Spain, and propose a causative role for SARS‐CoV‐2.
Patients and methods
We present a retrospective case series of paediatric patients diagnosed clinically and histopathologically with chilblains during the COVID‐19 pandemic. Approval from the institutional ethics committee and board was obtained. Standard informed consents were obtained for recording images and for skin biopsies in all patients.
The patients were seen in the emergency department and then referred to the dermatology department of a children’s hospital over a period of 4 weeks (April to May 2020), shortly after the peak of incidence of COVID‐19 in Madrid. Six of the patients (cases 1–6) were included in a previous report focused on the clinical and epidemiological features of 22 patients with similar lesions.1
Seven biopsy specimens from seven patients with skin lesions clinically diagnosed as COVID‐19‐related chilblains were examined. All of the biopsies were taken from lesions located on the feet or toes. Clinical parameters were recorded including age, sex, personal history of previous diseases, exposure to potentially infected household contacts, skin symptoms, location of lesions, systemic symptoms, therapies administered and follow‐up. Laboratory analyses performed were also recorded, as well as SARS‐CoV‐2 PCR from nasopharyngeal and oropharyngeal swabs.
All of the biopsies were assessed on multiple serial sections stained with haematoxylin and eosin, Mowry’s colloid iron and periodic acid–Schiff. The following histological features were recorded: vacuolar changes of the basal layer, exocytosis of lymphocytes, necrotic keratinocytes, erosion and ulceration of the epidermis, parakeratosis, spongiosis, oedema of the superficial dermis, perivascular superficial inflammatory infiltrate, perivascular deep inflammatory infiltrate, perieccrine lymphoid cell infiltrate, lymphocytic lobular panniculitis, fibrinoid material within the vessel walls, thrombi in papillary dermal vessels, thrombi in reticular dermis and subcutis vessels, lymphocytic infiltration of dermal vessels, purpura, dermal mucin, and basal membrane thickening. In each case, these features were scored as absent (−), mild/focal (+), moderate (++) or marked/extensive (+++).
Immunohistochemical stains with antibodies against CD3, CD4, CD8, CD20, CD30 and CD61 (Dako, Glostrup, Denmark) were performed in all of the samples. For SARS‐CoV and SARS‐CoV‐2 immunostains the tissue was cut from paraffin blocks in 3‐mm sections using a microtome and stretched on a water bath at 40 °C, mounted on glass slides and incubated at 60 °C for 1 h. The slides were deparaffinized in xylene and hydrated in ethanol. Antigen retrieval was performed with 10 mmol L−1 citrate buffer (pH 6.0) in a PT Link (Agilent Technologies, Santa Clara, CA, USA) at 95 °C for 20 min. We used a monoclonal antibody (1A9, dilution 1 : 200; GeneTex Inc., Irvine, CA, USA) against the spike protein of SARS‐CoV and SARS‐CoV‐2. The staining was visualized with the chromogenic substrate 3‐amino‐9‐ethylcarbazole [Dako EnVision+ System – HRP (AEC); Agilent Technologies] for 4 min, counterstained with Mayer’s haematoxylin, and mounted with commercially ready‐to‐use Dako Ultramount Aqueous Permanent Mounting Medium. The staining was carried out with a Dako Autostainer Link 48 (Agilent Technologies). Negative controls (tonsils from patients without COVID‐19) were included together with each sample. The antibody was previously optimized using sections of lungs from autopsies of patients with COVID‐19 as positive controls and different inflammatory skin conditions as negative controls.
We evaluated the relative proportion of T and B cells, the proportion of helper to cytotoxic T cells and the presence of activated lymphocytes. The presence and location of the virus were recorded as present (+) or absent (−). CD61 was examined to highlight the presence (+) or absence (−) of intravascular platelet thrombi. Transmission electron microscopy examination was performed in case 2.
All of the morphological, histochemical and immunohistochemical parameters were assessed by two of the authors (I.C. and A.T.) and SARS‐CoV‐ and SARS‐CoV‐2‐stained slides were seen by four (I.C., A.T., L.R. and C.S.).
Results
Clinical features
Our seven patients (four male, three female; 11–17 years old) had skin lesions on the toes and lateral aspects of their feet and heels that were consistent with chilblains (Figure 1). They were minimally painful or pruritic. The hands were also affected in one patient, who had associated lesions of erythema multiforme on the elbows and knees.7 Of note, no patient had a history of rheumatic disease, lupus erythematosus, Raynaud phenomenon, acrocyanosis or previous chilblains, and two of them were on treatment with methylphenidate hydrochloride for more than 1 year at the same dose for attention deficit hyperactivity disorder. The lesions had been present for 4–30 days before the biopsy procedure (Table 1). In all patients, the lesions had a benign outcome, with no significant systemic complaints, and gradual spontaneous resolution was achieved in all of them after 8 weeks of follow‐up.
Figure 1.

(a, b) Case 2 and (c, d) case 6. Clinical spectrum of perniotic acral ischaemic lesions.
Table 1.
Clinical features in seven children and adolescents with COVID‐19 chilblains
| Case | Age (years) | Sex | ADHD | Suspected household contact | Respiratory/GI symptoms | Time to biopsy | Site of lesions | Local symptoms | PCR |
| 1 | 11 | F | No | Yes | Yes/yes | 4 days | Feet | − | − |
| 2 | 13 | F | Yes | No | Yes/no | 11 days | Feet | Mild pain | − |
| 3 | 15 | F | No | No | Yes/no | 30 days | Feet | − | NA |
| 4 | 15 | M | No | Yes | No/no | 15 days | Feet | − | − |
| 5 | 14 | M | No | No | Yes/no | 20 days | Feet | Pruritus | − |
| 6 | 17 | M | No | Yes | Yes/no | 20 days | Feet, hands | Pruritus | − |
| 7 | 15 | M | Yes | Yes | No/no | 7 days | Feet | Pruritus | − |
ADHD, attention deficit hyperactivity disorder; F, female; GI, gastrointestinal; M, male; NA, not available; PCR, polymerase chain reaction. ‘−’ indicates a negative result.
SARS‐CoV‐2 PCR from nasopharyngeal and oropharyngeal swabs was negative in all cases tested (six of six). PCR tests were performed between 1 and 21 days (median 10) from the beginning of the skin lesions. Coagulation studies were normal in six patients tested. D‐dimer levels in serum were measured in six cases and were minimally elevated in one case (900 ng mL−1; normal < 500 ng mL−1), but this abnormal result had no clinical significance, with the patient showing good health, no systemic symptoms and other coagulation tests within normal limits. Full blood count was normal in all tested cases.
Histopathology
The biopsies showed similar findings with variable intensity (Table 2). All showed a mild interface dermatitis featuring vacuolar degeneration of the basal epidermal layer. Exocytosis of lymphocytes was seen in three cases and scattered necrotic keratinocytes in four. Lymphocytic vasculitis was demonstrated in all biopsies. Lymphocytes infiltrated the wall of dermal venules and arterioles. Endotheliitis, defined as swollen endothelial cells separated from the underlying basement membrane by subendothelial lymphocytes, was frequently observed (Figure 2). Indirect features of vascular damage such as red cell extravasation and dermal oedema were present in all cases. Fibrinoid necrosis of vessels was seen in two biopsies and microthrombosis in four. These thrombi were noted in papillary dermal capillaries and also involved reticular dermis vessels (Figure 3). Transmural lymphocytic infiltration of a large subcutaneous vessel, not associated with fibrinoid necrosis or thrombosis, was noted in one case.
Table 2.
Histopathological features of seven skin biopsies of COVID‐19 chilblains in children and adolescents
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | Case 7 | |
| Basal vacuolar changes | + | ++ | ++ | + | + | + | + |
| Exocytosis | − | ++ | − | + | − | + | − |
| Necrotic keratinocytes | + | + | + | − | − | + | − |
| Erosion or ulceration | − | − | − | − | − | − | − |
| Parakeratosis | − | + | − | ++ | ++ | − | + |
| Spongiosis | + | ++ | + | + | + | ++ | + |
| Dermal oedema | + | ++ | ++ | ++ | + | ++ | + |
| Perivascular superficial inflammation | + | +++ | +++ | + | + | + | + |
| Perivascular deep inflammation | + | +++ | +++ | + | + | ++ | + |
| Perieccrine inflammation | + | +++ | +++ | + | + | ++ | NA |
| Lymphocytic panniculitis | + | +++ | +++ | + | + | + | NA |
| Fibrinoid necrosis | − | + | + | − | − | − | − |
| Thrombi in superficial dermis | − | + | − | − | − | − | − |
| Thrombi in deep dermis | − | + | + | + | + | − | − |
| Lymphocytic infiltration of vessels | + | +++ | +++ | + | + | ++ | + |
| Purpura | + | +++ | + | + | + | ++ | + |
| Dermal mucin | − | + | ++ | + | + | + | − |
| Basal membrane thickening | − | − | − | − | − | − | − |
| Other findings | Vascular ectasia | − | − | Vascular ectasia | − | Subcutaneous lymphocytic vasculitis | Vascular ectasia |
Features were scored as absent (−), mild/focal (+), moderate (++) or marked/extensive (+++), or were not assessable (NA).
Figure 2.
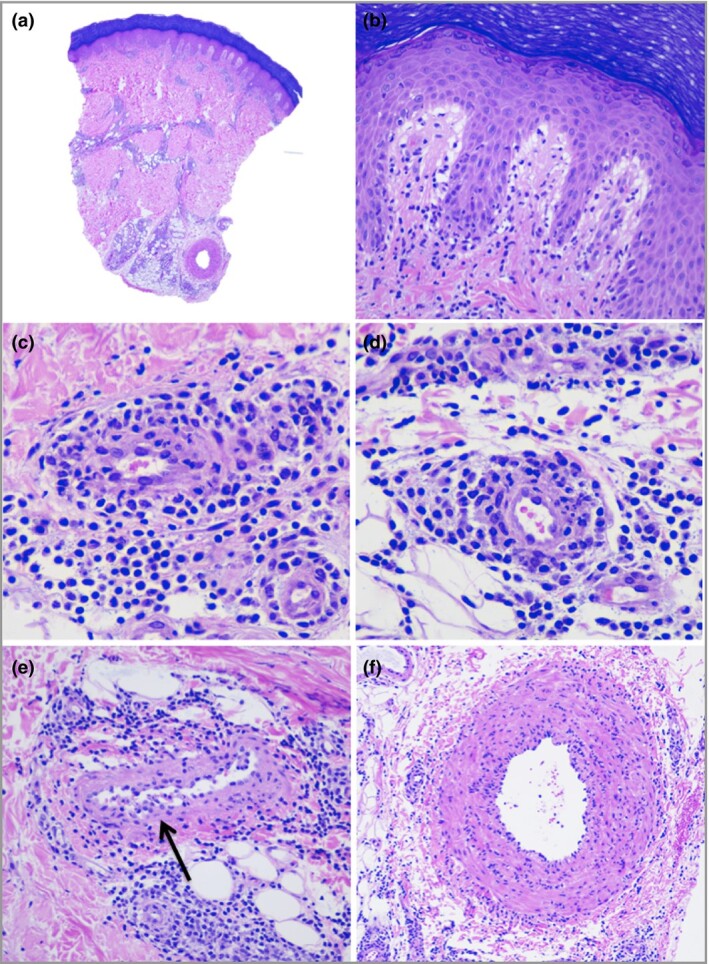
Case 6, skin biopsy. (a) Acral skin showing superficial and deep perivascular inflammation extending into the subcutis and papillary dermal oedema [haematoxylin and eosin (H&E), original magnification × 20]. (b) Mild exocytosis and vacuolar degeneration (H&E, × 200). (c–f) Lymphocytic infiltration of vessel walls. Note the lifting of endothelium with underlying lymphocytes in (e) (arrow) and transmural inflammation of a large subcutaneous vessel in (f). H&E, original magnification (c, e) × 400; (d, f) × 200.
Figure 3.
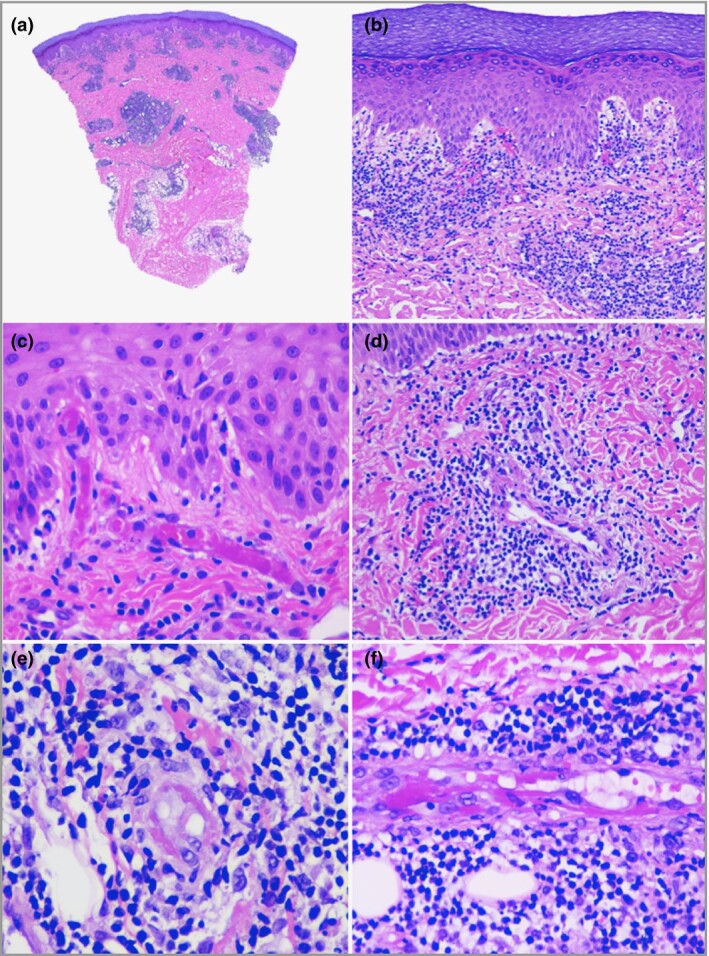
Case 2, skin biopsy. (a) Acral skin showing superficial and deep perivascular inflammation extending into the subcutis [haematoxylin and eosin (H&E), original magnification × 20]. (b) Mild papillary dermal oedema, vacuolar degeneration of the basal layer and lymphocytic exocytosis together with prominent red cell extravasation (H&E, × 100). (c) Thrombi in superficial dermis vessels (H&E, × 200). (d–f) Lymphocytic vasculitis with thrombosis and fibrin deposition in vessel walls. H&E, original magnification (d) × 200, (e, f) × 400.
A superficial and deep angiocentric and eccrinotropic lymphocytic infiltrate was seen in all samples. Inflammation extended to the subcutaneous fat in the six biopsies where the subcutis was represented and involved mostly the fat lobule. The inflammatory infiltrate was predominantly composed of small lymphocytes. Large activated lymphocytes were noted in only two cases (cases 2 and 3) with more severe inflammation. Plasma cells were only focally seen in these two biopsies showing more dense inflammation.
Immunohistochemistry
The inflammatory infiltrate was predominantly composed of mature T cells (CD3+) with a predominance of helper T lymphocytes (CD4+) over cytotoxic T lymphocytes (CD8+). Only scattered mature B lymphocytes (CD20+) were seen, except for case 5, where aggregates of B cells were noted in the centre of dense nodular lymphoid nodules. Scattered CD30+ cells were observed in cases 2 and 3. CD61 highlighted the presence of small microthrombi in four cases, including ones where thrombi were not apparent on haematoxylin and eosin‐stained sections (case 6) (Table 3).
Table 3.
Summary of immunohistochemical findings
| Case | Inflammatory cell phenotype | CD4 : CD8 ratio | Thrombi on CD61 | SARS‐CoV‐2 spike protein |
| 1 | Mainly CD3+, scattered CD20+ | 4 : 1 | − | + |
| 2 | Mainly CD3+, scattered CD20+ and CD79+, scattered CD30+ | 1 : 1 | + | + |
| 3 | Mainly CD3+, aggregates of CD20+ and CD79a+, scattered CD30+ | 2 : 1 | − | + |
| 4 | Mainly CD3+, scattered CD20+ and CD79a+ | 2 : 1 | + | + |
| 5 | Mainly CD3+, scattered CD20+ and CD79a+ | 3 : 1 | + | + |
| 6 | Mainly CD3+, scattered CD20+ and CD79a+ | 3 : 1 | + | + |
| 7 | Mainly CD3+, scattered CD20+ | 2 : 1 | − | + |
Cytoplasmic granular positivity for SARS‐CoV‐2 spike protein was mainly demonstrated in endothelial cells of the capillary and postcapillary venules of the upper dermis, and also in epithelial cells of the secretory portion of eccrine units in all cases (Figure 4a–c).
Figure 4.
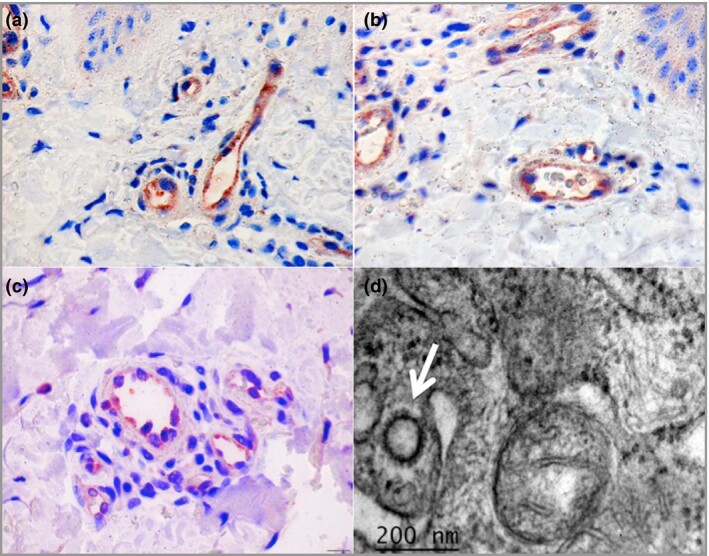
(a–c) Cases 4–6. Cytoplasmic granular positivity for SARS‐CoV‐2 spike protein in endothelial cells (immunohistochemistry, original magnification × 400). (d) Case 2. Ultrastructural image of an endothelial cell showing coronavirus‐like particles consistent with SARS‐CoV‐2 (arrow), next to a mitochondrion for size comparison (electron microscopy, × 60 000).
Electron microscopy
Ultrastructural examination revealed the presence of round membrane‐bound structures within the cytoplasm of endothelial cells showing an electrolucent centre, and surrounded by tiny spikes, giving them a halo‐like appearance. Their mean diameter was 92.26 nm (range 80.76–109.76) and the mean thickness of the spikes was 13.18 nm (range 12.36–13.88). Based on previous descriptions in the literature, these structures were interpreted as coronavirus‐like particles8–14 (Figure 4d). Tubuloreticular inclusions were also found within the endothelial cells, similarly to other descriptions of SARS‐CoV‐2 and SARS‐CoV infections.8, 15
Discussion
Lymphocytic vascular damage was the hallmark feature in biopsies from our seven patients with COVID‐19‐related chilblains. The intensity of the vasculitic damage ranged from minor findings, such as endothelial cell tumefaction and mild lymphocytic infiltration of the walls, to more severe signs like fibrinoid necrosis and thrombosis. The spectrum of histopathological features did not correlate with the duration of the lesions.
Vasculitis is defined as inflammation directed at vessels, which compromises or destroys the vessel wall leading to haemorrhagic and ischaemic events. The spectrum of vascular reaction to injury is variable.16 Moderate‐to‐severe lymphocytic inflammation of vessel walls was noted in half of our cases, and inflammation was mild in the rest. In all of them, even in those with mild inflammatory infiltrate, indirect evidence of vascular damage and leakage was present in the form of extravasation of erythrocytes and dermal oedema.
The overall clinical and histopathological features in our cases are entirely in keeping with chilblains. Biopsies of chilblains show a moderate‐to‐dense superficial and deep perivascular lymphocytic infiltrate with exocytosis to the epidermis and acrosyringia and perieccrine accentuation. A few necrotic keratinocytes and mild vacuolar degeneration of the basal layer can be observed occasionally. Pronounced papillary dermal oedema and spongiosis are often present. Lymphocytic vasculitis is a common feature, and superficial thrombosis is present in some cases. Chilblains may be classified as primary (idiopathic, cold related) or secondary to underlying conditions. Some authors consider that primary and secondary chilblains cannot be reliably differentiated based only on microscopic features.17 Perieccrine inflammation and marked dermal oedema have been described as features favouring idiopathic chilblains over chilblains associated with connective tissue diseases, particularly lupus erythematosus, which is favoured by more prominent changes of interface dermatitis.18, 19 Immunohistochemistry for lymphoid markers is not useful in the differential diagnosis of primary and secondary chilblains, as both show a predominance of mature T cells with only a minor proportion of B cells and some histiocytes. Increased numbers of large CD30+ cells have been described in some cases of idiopathic chilblains, with no clinical significance.20, 21
Secondary causes of chilblains include connective tissue diseases (lupus erythematosus, Behçet disease, antiphospholipid syndrome, rheumatoid arthritis, Sjögren syndrome); cryopathies; haematoproliferative or neoplastic diseases; blood hyperviscosity states; genetic diseases (familial chilblain lupus, STING‐associated vasculopathy of infantile onset, Aicardi–Goutières syndrome, and interleukin‐1 receptor‐associated kinase‐4 deficiency); and anorexia or other disorders causing weight reduction.22–24 None of these causes of secondary chilblains was present in our patients. Moreover, cold exposure was unlikely to be the trigger in our cases, as all lesions appeared during the mild spring climate in Madrid.
A causal relationship with COVID‐19 has been considered doubtful in this outbreak of cases of chilblains. However, we are not surprised by the high rate of negative PCR tests in our cases considering the reported low rate of positive PCR tests in children with symptoms suggestive of COVID‐19.25 We have demonstrated the presence of viral particles within endothelial cells in lesional skin biopsies from patients presenting with chilblains during the COVID‐19 pandemic. The positive immunohistochemistry was confirmed by the presence of viral particles in one case using transmission electron microscopy. Our results strongly support a pathogenetic role for SARS‐CoV‐2 in chilblains presenting during the pandemic. COVID‐19 should be included in the list of secondary causes of chilblains, and we think these lesions can be denominated from now onwards as COVID‐19 chilblains.
It has been proposed that SARS‐CoV‐2 uses angiotensin‐converting enzyme (ACE)2 expressed by pneumocytes in the epithelial alveolar lining to infect the host cells and cause lung injury.26, 27 It is likely that SARS‐CoV‐2 uses ACE2 to enter vessels, as ACE2 is widely expressed by endothelial cells.28, 29 ACE2 is also present in epithelial cells of eccrine glands, explaining the positive immunolocalization of SARS‐CoV‐2 we have observed in these cells.29
Vascular injury and thrombosis could explain the clinical features of chilblains and related acroischaemic lesions seen in some patients with COVID‐19. Different mechanisms of vascular damage in this setting have been proposed. Varga et al.8 suggested that recruitment of immune cells, either by direct viral infection of the endothelium or immune mediated, can result in widespread endothelial dysfunction associated with apoptosis. Magro et al.30 demonstrated a pattern of tissue damage consistent with complement‐mediated microvascular injury in the lung and skin of five individuals with severe COVID‐19. Their findings provide a foundation for further exploration of the pathophysiological importance of complement in COVID‐19 and could suggest targets for specific intervention.
Histological features of COVID‐19‐related chilblains have been only scarcely described.5, 31 Kolivras et al.5 reported a SARS‐CoV‐2 PCR‐positive 23‐year‐old man with mild systemic symptoms and skin lesions suggestive of chilblains on his feet and toes. A skin biopsy showed features consistent with chilblains, and the authors suggested a possible role for interferon‐1, based on the similarities with chilblain lupus erythematosus. The presence of SARS‐CoV‐2 particles in endothelial cells in our cases argues against this hypothesis, suggesting SARS‐CoV‐2 as a direct cause of the endothelial damage and thrombosis instead. A primary thrombotic mechanism appears unlikely for COVID‐19 chilblains based on the limited presentation and normal coagulation tests.
Chilblains seen in young people may, to some extent, resemble the severe acral ischaemia caused by thrombosis in severely ill patients with COVID‐19. These patients are usually elderly and admitted to intensive care units, and show coagulopathy with very elevated D‐dimer levels.32 A severity spectrum cannot be ruled out as widespread endothelial infection could contribute to the systemic multiorgan manifestations seen in patients with severe COVID‐19. In fact, SARS‐CoV‐2 has been shown to infect endothelial cells in the skin and other organs in a few cases.8, 30, 33
Our study has some potential limitations. We acknowledge that the number of patients is small; furthermore, evidence of SARS‐CoV‐2 infection by PCR and serology could not be obtained. Also, the use of immunohistochemistry for SARS‐CoV and SARS‐CoV‐2 is still restricted and larger studies are necessary to assess with accuracy the role of immunohistochemistry in the diagnosis of COVID‐19. Finally, we only carried out electron microscopy in one case; even though the virus was detected, more cases are needed to support our conclusions further.
In conclusion, the presence of SARS‐CoV‐2 in the endothelium of dermal vessels in skin biopsies of children and adolescents with acute chilblains confirms that these lesions are a manifestation of COVID‐19. Their clinical and histopathological features are similar to those of chilblains of other aetiologies, and virus‐induced vascular damage could explain their pathophysiology. Our findings support the hypothesis that widespread endothelial infection by SARS‐CoV‐2 could have a role in the pathogenesis of severe forms of the disease. More studies are needed to understand the reasons why previously healthy children, adolescents and young adults present with limited skin forms of COVID‐19, in contrast with the severe multiorgan presentations seen in older patients with background diseases.
Acknowledgments
The authors want to thank Dr Sandra Pérez‐Buira, Ms Raquel Pajares‐Martinez, Ms Ana Sanz‐Miguel, Ms Ainhoa Iparraguirre‐Diaz and Ms Maria Paz Fernandez‐Lopez for their technical assistance performing the immunohistochemical stains, and Dr Victor Quintero for his critical review and useful suggestions on improving the manuscript.
Contributor Information
I. Colmenero, Department of Pathology Hospital Infantil Universitario Niño Jesús Madrid Spain.
C. Santonja, Department of Pathology Hospital Universitario Fundación Jiménez Díaz Madrid Spain
M. Alonso‐Riaño, Department of Pathology Hospital Universitario 12 de Octubre Madrid Spain
L. Noguera‐Morel, Department of Dermatology Hospital Infantil Universitario Niño Jesús Madrid Spain
A. Hernández‐Martín, Department of Dermatology Hospital Infantil Universitario Niño Jesús Madrid Spain
D. Andina, Emergency Department Hospital Infantil Universitario Niño Jesús Madrid Spain
T. Wiesner, Department of Dermatology Medical University of Vienna Vienna Austria
J.L. Rodríguez‐Peralto, Department of Pathology Hospital Universitario 12 de Octubre Madrid Spain
L. Requena, Department of Dermatology Hospital Universitario Fundación Jiménez Díaz Madrid Spain
A. Torrelo, Department of Dermatology Hospital Infantil Universitario Niño Jesús Madrid Spain
References
- Andina D, Noguera‐Morel L, Bascuas‐Arribas M et al. Chilblains in children in the setting of COVID‐19 pandemic. Pediatr Dermatol 2020; 37:406–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- López‐Robles J, de la Hera I, Pardo J et al. Chilblain‐like lesions: a case series of 41 patients during the COVID‐19 pandemic. Clin Exp Dermatol 2020; DOI: 10.1111/ced.14275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galván Casas C, Català A, Carretero Hernández G et al. Classification of the cutaneous manifestations of COVID‐19: a rapid prospective nationwide consensus study in Spain with 375 cases. Br J Dermatol 2020; 183:71–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BBC News. Coronavirus: ‘Covid toe’ and other rashes puzzle doctors. Available at: https://www.bbc.com/news/health‐52493574 (last accessed 20 July 2020).
- Kolivras A, Dehavay F, Delplace D et al. Coronavirus (COVID‐19) infection‐induced chilblains: a case report with histopathologic findings. JAAD Case Rep 2020; 18:489–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Colonna C, Monzani NA, Rocchi A et al. Chilblains‐like lesions in children following suspected Covid‐19 infection. Pediatr Dermatol 2020; 37:437–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torrelo A, Andina D, Santonja C et al. Erythema multiforme‐like lesions in children and COVID‐19. Pediatr Dermatol 2020; 37:442–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varga Z, Flammer AJ, Steiger P et al. Endothelial cell infection and endotheliitis in COVID‐19. Lancet 2020; 395:1417–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varga Z, Flammer AJ, Steiger P et al. Electron microscopy of SARS‐CoV‐2: a challenging task – authors’ reply. Lancet 2020; 395:e100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldsmith CS, Miller SE, Martines RB et al. Electron microscopy of SARS‐CoV‐2: a challenging task. Lancet 2020; 395:e99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Su H, Yang M, Wan C et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID‐19 in China. Kidney Int 2020; 98:219–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kissling S, Rotman S, Gerber C et al. Collapsing glomerulopathy in a COVID‐19 patient. Kidney Int 2020; 98:228–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhu N, Zhang D, Wang W et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 2020; 382:727–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Menter T, Haslbauer JD, Nienhold R et al. Post‐mortem examination of COVID19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings of lungs and other organs suggesting vascular dysfunction. Histopathology 2020; DOI: 10.1111/his.14134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldsmith CS, Tatti KM, Ksiazek TG et al. Ultrastructural characterization of SARS coronavirus. Emerg Infect Diseases 2004; 10:320–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlson JA. The histological assessment of cutaneous vasculitis. Histopathology 2010; 56:3–23. [DOI] [PubMed] [Google Scholar]
- Crowson AN, Magro CM. Idiopathic perniosis and its mimics: a clinical and histological study of 38 cases. Hum Pathol 1997; 28:478–84. [DOI] [PubMed] [Google Scholar]
- Cribier B, Djeridi N, Peltre B et al. A histologic and immunohistochemical study of chilblains. J Am Acad Dermatol 2001; 45:924–9. [DOI] [PubMed] [Google Scholar]
- Boada A, Bielsa I, Fernández‐Figueras MT et al. Perniosis: clinical and histopathological analysis. Am J Dermatopathol 2010; 32:19–23. [DOI] [PubMed] [Google Scholar]
- Massey PR, Wanat KA, Stewart CL et al. CD30 positive atypical lymphocytes in perniosis: a potential histopathologic pitfall in a benign condition. Am J Dermatopathol 2014; 36:730–3. [DOI] [PubMed] [Google Scholar]
- Wang ML, Chan MP. Comparative analysis of chilblain lupus erythematosus and idiopathic perniosis: histopathologic features and immunohistochemistry for CD123 and CD30. Am J Dermatopathol 2018; 40:265–71. [DOI] [PubMed] [Google Scholar]
- Cappel JA, Wetter DA. Clinical characteristics, etiologic associations, laboratory findings, treatment, and proposal of diagnostic criteria of pernio (chilblains) in a series of 104 patients at Mayo Clinic, 2000 to 2011. Mayo Clin Proc 2014; 89:207–15. [DOI] [PubMed] [Google Scholar]
- Gurung P, Lee ASW, Armon K et al. Chilblains accompanying interleukin‐1 receptor‐associated kinase (IRAK)‐4 deficiency. Clin Exp Dermatol 2018; 43:596–7. [DOI] [PubMed] [Google Scholar]
- Lutz V, Cribier B, Lipsker D. Chilblains and antiphospholipid antibodies: report of four cases and review of the literature. Br J Dermatol 2010; 163:645–6. [DOI] [PubMed] [Google Scholar]
- Tagarro A, Epalza C, Santos M et al. Screening and severity of coronavirus disease 2019 (COVID‐19) in children in Madrid, Spain. JAMA Pediatr 2020; DOI: 10.1001/jamapediatrics.2020.1346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perrotta F, Matera MG, Cazzola M et al. Severe respiratory SARS‐CoV2 infection: does ACE2 receptor matter? Respir Med 2020; 168:105996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shang J, Wan Y, Luo C et al. Cell entry mechanisms of SARS‐CoV‐2. Proc Natl Acad Sci U S A 2020; 117:11727–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- To KF, Lo AWI. Exploring the pathogenesis of severe acute respiratory syndrome (SARS): the tissue distribution of the coronavirus (SARS‐CoV) and its putative receptor, angiotensin‐converting enzyme 2 (ACE2). J Pathol 2004; 203:740–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamming I, Timens W, Bulthuis MLC et al. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol 2004; 203:631–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Magro C, Mulvey JJ, Berlin D et al. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID‐19 infection: a report of five cases. Transl Res 2020; 220:1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Masson A, Bouaziz J‐D, Sulimovic L et al. Chilblains are a common cutaneous finding during the COVID‐19 pandemic: a retrospective nationwide study from France. J Am Acad Dermatol 2020; 83:667–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suarez‐Valle A, Fernandez‐Nieto D, Diaz‐Guimaraens B et al. Acro‐ischemia in hospitalized COVID‐19 patients. J Eur Acad Dermatol Venereol 2020; DOI: 10.1111/jdv.16592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ackermann M, Verleden SE, Kuehnel M et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid‐19. N Engl J Med 2020; 383:120–8. [DOI] [PMC free article] [PubMed] [Google Scholar]