
FIGURE 10.
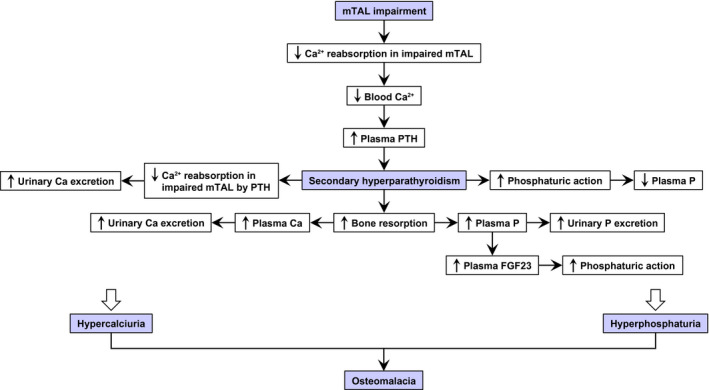
Mechanism underlying the changes in calcium (Ca) and phosphate (P) homeostasis over time in GlatmTg(CAG‐A4GALT) mice with osteomalacia due to secondary hyperparathyroidism. GlatmTg(CAG‐A4GALT) mice were characterized by progressive medullary thick ascending limb (mTAL) impairment without remarkable damage to the glomeruli or proximal tubule (PTs). 18 Generally, 20%–25% of filtered Ca2+ is reabsorbed in the TAL, while very low levels of filtered P are reabsorbed. 30 Parathyroid hormone (PTH) increases phosphaturic action in PTs, which is evidenced by a decrease in P reabsorption and increase in P excretion. PTH increases reabsorption of Ca2+ in the TAL, 30 decreasing Ca excretion. In GlatmTg(CAG‐A4GALT) mice, mTAL impairment leads to insufficient Ca2+ reabsorption. 18 Low blood Ca2+ (Figure 4A) elevated plasma PTH levels by 5 wk of age (Figure 5A), showing progressively increased phosphaturic action, ie, decreased P reabsorption in the unimpaired PT and increased urinary P excretion (Figure 4C), and decreased plasma P levels at 10 wk of age (Figure 4B). Secondary hyperparathyroidism developed by 20 wk of age (Figure 5A) and increased bone resorption (Figure 2D), leading to hyperphosphatemia (Figure 4B), which increases urinary P excretion (Figure 4C) and plasma FGF‐23 levels (Figure 5B) with phosphaturic action. Despite the increasing plasma PTH levels (Figure 5A), the progressively impaired mTAL exhibited insufficient urinary Ca reabsorption, leading to increased Ca excretion over time. 18 Bone resorption (Figure 2D) caused hypercalcemia, 18 which increased urinary Ca excretion. 18 Thus, hyperphosphaturia and hypercalciuria result in osteomalacia in GlatmTg(CAG‐A4GALT) mice. FGF‐23, fibroblast growth factor 23