
Figure 1. A Case of Disseminated Coccidioidomycosis Characterized by Defective Interleukin-12 Signaling and Th1 Response.
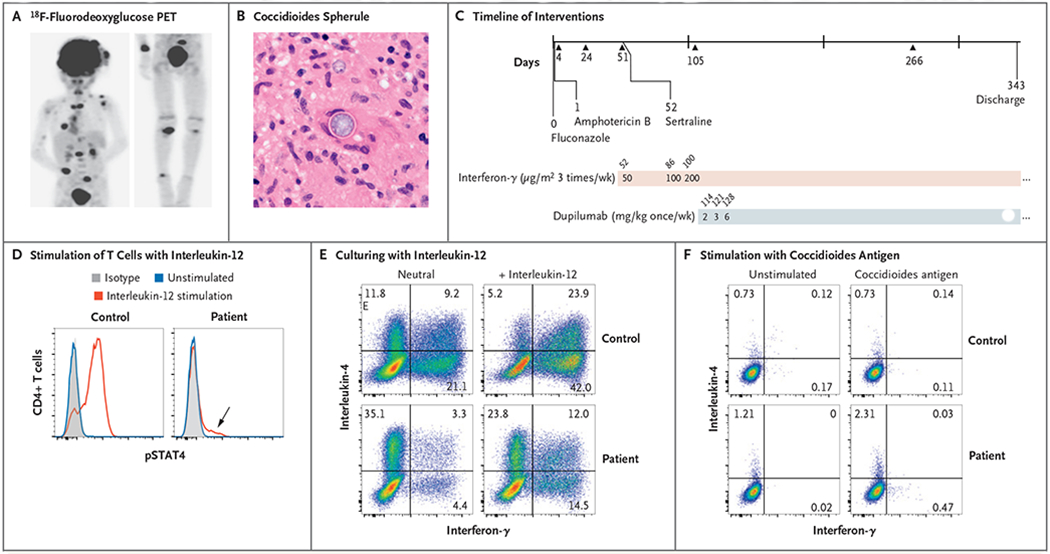
Panel A shows an 18F-fluorodeoxyglucose positron-emission tomographic scan showing disseminated infection with multiple lesions of the spine, clavicle, ribs, paratracheal lymph nodes, right distal radius, and right leg. Panel B shows a coccidioides spherule obtained from surgical biopsy of a scalp lesion. Panel C shows the timeline of interventions in our patient. Initial treatment included fluconazole and liposomal amphotericin B, and sertraline was added at day 52 after admission. Treatment with subcutaneous interferon-γ was also started on day 52, and treatment with dupilumab was started on day 114. Triangles represent major debridement surgical procedures. Doses of interferon-γ and dupilumab are indicated in the shaded bars; numbers above the bars are days after admission. Panel D shows stimulation of helper T cells with interleukin-12, which led to a poor phosphorylated STAT4 (pSTAT4) response; however, the loss of function was not absolute (arrow). Panel E shows intracellular cytokine staining of CD4+ T-cell effectors generated in neutral conditions and stimulated with phorbol myristate acetate (PMA) and ionomycin. Interleukin-4 production was greatly enhanced relative to interferon-γ production in the patient as compared with a control. A normal response was only partially restored by culturing in type 1 helper T (Th1) cell conditions (i.e., with interleukin-12). Panel F shows stimulation of peripheral-blood mononuclear cells with T27K coccidioidal antigen, which led to increased production of interleukin-4 over interferon-γ in helper T cells.