
Figure 2. Theoretical model of thyroid-associated ophthalmopathy (TAO) pathogenesis.
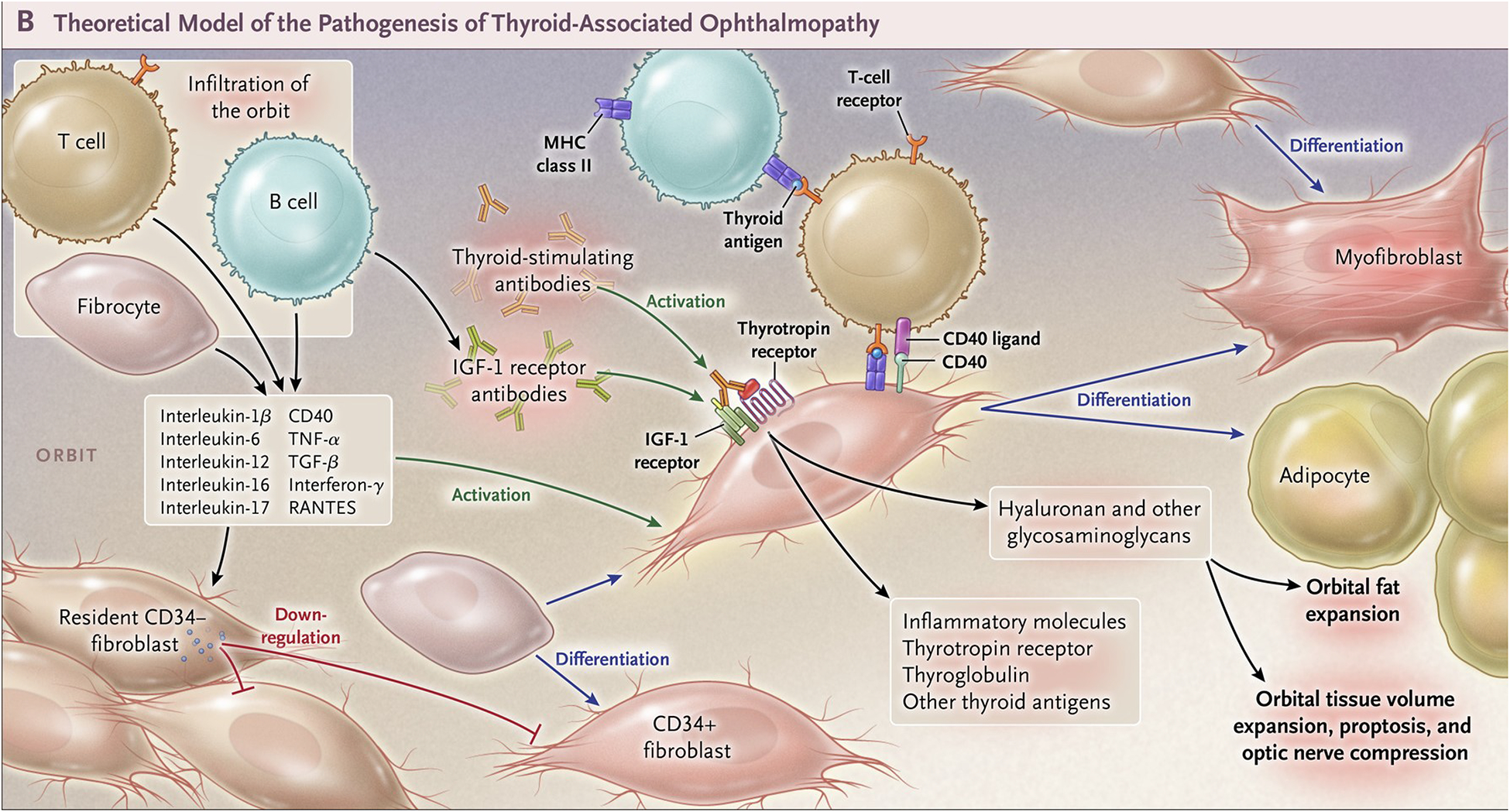
CD34+ fibrocytes, monocyte-derived progenitor cells coming from the bone marrow, circulate in Graves’ disease at higher abundance than in healthy control individuals. Fibrocytes express the thyrotropin receptor (TSHR), thyroglobulin, thyroperoxidase and sodium-iodide symporter. They constitutively express Class II major histocompatibility complex (MHC) and present antigens to T cells. They can differentiate into CD34+ fibroblasts, myofibroblasts, and adipocytes. Many of the genes expressed by fibrocytes are detected at considerably lower levels in CD34+ fibroblasts. When activated, CD34+ fibroblasts generate several pro-inflammatory or anti-inflammatory cytokines, including interleukins 1β, 6, 8, 10, 12, 16, tumor necrosis factor α, and regulated on activation, normal T expressed and secreted (RANTES), CXCL-12 and CD40-CD154. Orbital fibroblasts display insulin-like growth factor-I receptor (IGF-IR) on their cell surfaces. Orbital fibroblasts express three mammalian hyaluronan synthase isoenzymes and UDP glucose dehydrogenase and synthesize hyaluronan, the glycosaminoglycan associated with expanding orbital tissue in TAO. From N. Engl. J. Med, Smith T.J. and Hegedus L., Graves’ Disease, 375; 1552–1565. Copyright © (2016) Massachusetts Medical Society. Reprinted with permission.