

Abstract
Emerging pandemics show that humans are not infallible and communities need to be prepared. Coronavirus outbreak was first reported towards the end of 2019 and has now been declared a pandemic by the World Health Organization. Worldwide countries are responding differently to the virus outbreak. A delay in detection and response has been recorded in China, as well as in other major countries, which led to an overburdening of the local health systems. On the other hand, some other nations have put in place effective strategies to contain the infection and have recorded a very low number of cases since the beginning of the pandemics. Restrictive measures like social distancing, lockdown, case detection, isolation, contact tracing, and quarantine of exposed had revealed the most efficient actions to control the disease spreading. This review will help the readers to understand the difference in response by different countries and their outcomes. Based on the experience of these countries, India responded to the pandemic accordingly. Only time will tell how well India has faced the outbreak. We also suggest the future directions that the global community should take to manage and mitigate the emergency.
Keywords: COVID-19, OneHealth, pandemic, SARS-Cov-2
On December 31, 2019, hospitals in Wuhan, Hubei province, China reported on a cluster of cases suffering from pneumonia of unknown cause, attracting global attention.[1] Two weeks later, a new variant of coronavirus was identified, which was named 'severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).[2] SARS-CoV-2 is part of a group of viruses in a format similar to the crown (Corona), more specifically belonging to the species Betacoronavirus, such as the Middle East respiratory syndrome coronavirus (MERS-CoV) and severe acute respiratory syndrome coronavirus (SARS-CoV). Over the next few weeks, it spread to18 countries (excluding China), and on January 30, 2020, the World Health Organization (WHO) declared the outbreak to be a Public Health Emergency of International Concern (PHEIC). Subsequently, on March 11th, it was declared a pandemic as it had spread to 113 countries.[2] As of March 31, 2020, baring a few, almost all countries and more than a million people are affected [Fig. 1]. In terms of fatality, though the case fatality rate of SARS-CoV-2 is 3.44%, lower than MERS-CoV (34.4%) and SARS-CoV (9.19%), the absolute numbers affected are more.[3]
Figure 1.
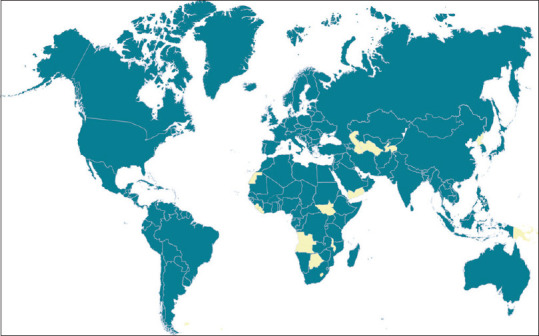
Countries, territories, and areas with reported confirmed cases of COVID-19, 31st March 2020[2]
SARS versus SARS-CoV-2
SARS outbreak took place in 2002 in China and infected 8,422 people globally.[4] The total number of deaths was 916 globally.[4] As of March 31, 2020, the SARS-CoV-2 has infected over a million and has caused more than 50,000 deaths.[2] One reason why its spread is evidently much wider as compared to SARS is the rapid urbanization and the increase in international travel during the last two decades. Hence, the control measures applied at the time of SARS are no longer adequate in these days, and more vigorous actions are required to control SARS-CoV-2.[5] Another reason is related to a difference in the infectious period between patients infected with SARS and those infected with SARS-CoV-2. While in the former case, viral shedding peaks only when the patient's illness is advanced and respiratory symptoms occur,[5] for SARS-CoV-2, transmission can occur in the early phase of the illness, when the patients are completely asymptomatic.[6,7] Hence, isolation after the onset of symptoms might be ineffective in preventing virus transmission and this also makes temperature screening less effective.[8] Finally, SARS-CoV-2 has been proven to hold higher transmissibility and wider community spread than other betacoronaviridae.[5] Despite being highly infectious and having higher transmissibility, the severity of SARS-CoV-2 is much lesser compared to SARS.[5]
Containment Measures
Statistical models on the spread of SARS-CoV-2 suggested that, due to lack of herd immunity in the population and the highly contagious nature of the virus, 40-70% of the population can be infected unless strong containment measures are timely taken.[9] Based on the past experience with different epidemics and pandemics, as well as the current understanding of SARS-CoV-2, the WHO suggested frequent hand washing with an alcohol-based hand rub or soap and water, avoiding touching eyes, nose, and mouth, and practicing respiratory hygiene.[2] The use of face masks by everyone is still controversial, though WHO does not recommend its use by everyone.[2]
Coronavirus can survive on different surfaces for a long time – plastic (72 hours), stainless steel (48 hours), cardboard (24 hours), and copper (4 hours).[10,11] As regard to contact spreading, the virus can be effectively inactivated by surface disinfection with 70% isopropyl alcohol, 0.5% hydrogen peroxide, or 0.1% sodium hypochlorite.[10,11] Hence, thorough cleaning with disinfecting solutions in health facilities and public places is warranted. Health care facilities are advised to use personal protective equipment (PPE) with triple-layered masks or N95 masks and to educate the staff about the proper disposal of the equipment.[2] Respiratory precautions during aerosol-generating procedures are also recommended.[2] Anyone with fever, cough, and difficulty in breathing is advised to seek medical attention.[2] Social distancing (minimum one meter) is recommended both at individual and community levels.[2]
At the community level, the most important measures for reducing infection spread rely on case detection, isolation, and contact tracing of positive cases, followed by quarantine for those exposed. Other strategies include the closure of places of mass gathering, like schools, libraries, places of worship, malls, and cinemas, and the suspension of all social events, as sports, celebrations, and meetings. Temperature screening has been introduced at airports, railway stations, and bus stations, as well as the entrance of the main community buildings (like hospitals, banks, or law courts). The limitation of temperature screening is that it misses a significant number of asymptomatic carries, which has been estimated at around 46%.[8] In countries with a worse rate of infection, more restrictive measures have been put in place, like travel bans, reduction or interruption of both internal and overseas flights, and boundary closure; curfew and lockdown are also implemented.
All the aforementioned measures aim at reducing the rate of infection transmission, thus delaying the timing and lowering the height of the epidemic peak. These allow, from one side, gaining time for the healthcare system to prepare an efficient response to the pandemic, and, from the other side, the development of potential new treatments and vaccines. In Wuhan, it has been calculated that physical distancing with a staggered return to work at the beginning of April instead of March was the most effective strategy, with a projected reduction of the median number of infections by 92% (interquartile range (IQR) 66-97) and 24% (IQR 13-90) in mid-2020 and end-2020, respectively.[12]
Responses of Various Countries to COVID-19
A range of strategies has been adopted worldwide based on the population structure as well as the health care infrastructure of each country. One of the problems that have been faced is the delay in the implementation of measures. A model simulation by Lai Shengjie and Andrew Tatem predicted that if China had implemented control measures a week earlier, 67% of all cases could have been prevented; if implementation had been done at the beginning of January, it would have cut infection rate to 5%.[13] The events in Wuhan show that for at least three weeks after the first cases were reported, city authorities had been informed about the virus spreading but they issued orders to suppress the news. For instance, on January 18th, roughly six weeks after coronavirus started to spread in Wuhan, they allowed the city's Baibuting district to organize its traditional annual mass banquet. Of the 40,000 families attending, more than 28,000 got infected and more than 560 succumbed to the virus in the later weeks. Just a few days later, more than 5 million people had traveled out of Wuhan for the upcoming Spring festival, just before Wuhan imposed lockdown, thus spreading COVID-19 across other provinces of China and abroad. The elevated connectivity of Wuhan with other international airports such as Singapore, Japan, and Thailand, facilitated the rapid spread to bordering countries.[14,15]
On January 23rd, a 3-week lockdown was ordered to the entire Hubei province, along with some major cities like Beijing and Shanghai.[16] Outdoor activities were limited, with each citizen being permitted to go out for 30 minutes only on every second day.[17] All transports in and out of the city were prohibited. Mobile-phone data location from Chinese Internet giant Baidu was used to track people's moments as well as person to person contacts.[18] In Wuhan, where the infection rate was the highest, residents were required to measure and report their temperature daily. The mild and asymptomatic cases were quarantined in 'Fangcang' hospital as well as in public spaces such as stadiums and conference centers, which have been repurposed for medical care.[19] A 1,000-bedded hospital was built in a matter of 10 days to take care of patients with coronavirus.
Thanks to all these measures, a decline in the number of infected growth rate and an increase in its doubling time (from 2 to 4 days) was eventually achieved. The median daily reproduction number declined from 2.35 of January 16 to 1.05 of January 30.[20] Tian et al. estimated that the Wuhan shutdown slowed the dispersal of infection to other cities by 2.91 days (95%CI: 2.54-3.29), delaying epidemic growth elsewhere in China.[21] Other Chinese cities that early implemented preventive control measures reported 33.3% fewer cases in the first week of their outbreaks compared with cities that started control later.[21] The correlation between domestic air traffic and COVID-19 spread became weaker following lockdown.[17] Nevertheless, a study from Italy, China, and the United States found that the Wuhan travel quarantine delayed the overall epidemic progression by only 3 to 5 days in Mainland China, but had a greater effect at the international scale, where case export was reduced by nearly 80%.[22] However, with all these measures, China prevented cases from increasing by 67-fold, i.e. without these measures there would have been 8 million cases by the end of February.[13] However, replicating the Chinese model elsewhere turned out to be extremely challenging, as the measures implemented in Wuhan and the entire Hubei province of China far exceeded the classical definition of local confinement, lockdown, and isolation [Fig. 2].[17]
Figure 2.
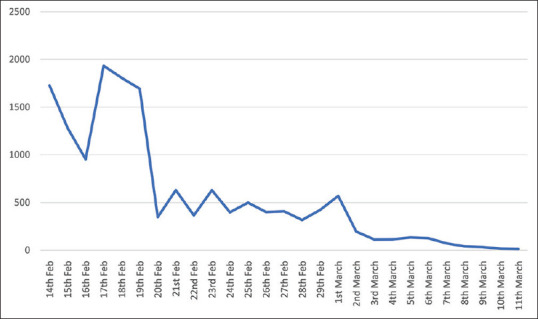
Number of new cases reported from the Hubei Province of China after the lockdown.[2]
Note: Hubei went for lockdown on January 23rd, 2020 and it took almost 6-8 weeks for the decline in new cases. Sudden decline on 20th February was related to change in definition from "Clinically Diagnosed" to "Suspected" and "Confirmed" cases, where the latter required laboratory diagnosis
Some of the other countries were successful in flattening the curve, including Singapore, Taiwan, Hong Kong, and South Korea. One of the key factors in the success of these countries was continuous testing, isolation of infected, and quarantining of contacts. In Singapore, temperature screening at the airport of all travelers arriving from Wuhan was started on January 3rd, even before identification of SARS-CoV-2 sequence. Aggressive contact tracing and quarantine of contacts of confirmed cases, travel advisories, and entry restrictions on people who had traveled to China in the preceding 14 days were implemented. At a community level, people were encouraged to work from home and to record their temperature twice a day; to make quarantine less onerous, the government offered self-employed people SGD $ 100 per day. Respiratory and hand hygiene and social distancing were followed rigorously.[23]
Temperature checking in all clinics and provision and use of PPE by medical staff were ordered as compulsory. Strict visitor controls, cohorting of patients with pneumonia or respiratory infection, and restriction of movement of patients and doctors between different healthcare institutions were also set up to prevent disease spread across multiple institutions. A network of 800 Public Health Preparedness clinics (PHPCs) was activated to enhance the management of respiratory infections in primary care settings. All pneumonia cases, severely-ill patients in intensive care units, deceased people with a possible infectious cause, and influenza-like illness (ILI) in primary care clinics were tested.[16,24]
Since February 7, 2020, the country has been in Disease Outbreak Response System Condition (DORSCON) Orange, the second-highest alert, signifying more relaxed measures of containment.[25] Besides Singapore, also Taiwan and Hong Kong were found well prepared before the outbreak, thus making a rapid and vigorous response to the first cases. Closure of places of mass gathering, travel restrictions and case detection, isolation and contact reducing (quarantine of exposed) were widely practiced. In South Korea, authorities called for voluntary social distancing and isolation. Apart from this, testing was scaled up aggressively (nearly 18,000 per day) and contact tracing was done through CCTV and credit card transactions. The general community was also encouraged to inform about infected people.[16]
In contrast, countries in Europe, like Italy, Spain, the United Kingdom, and the United States delayed implementing containment measures and failed in anticipating the impact of the pandemic in their own boundaries. Italy has recorded the highest number of deaths globally.[2] Before the outbreak was detected, the virus had been circulating into the country for at least 4 weeks. In just a matter of weeks (February 21 to March 22, 2020), Italy went from the discovery of the first official COVID-19 case to a state of complete lockdown.[26] Within this brief period, the impact on the country was nothing short of a tsunami. The health care system was literally overwhelmed with new pneumonia cases, with a considerable number of them in critical conditions. In the “red zone“ (i.e. the regions of Lombardia and Veneto, the most hit by the pandemic), the situation had become so grim that the risk of treating only those with a better prognosis (younger and healthier population) to the detriment of older people became almost reality.[27] The shortage of hospital beds, ventilators, and health professionals became a concrete threat. Health professionals from different disciplines (including Ophthalmology) were converted to COVID-19 patient care and who came in contact with SARS-CoV-2 patients were encouraged to work until they show symptoms.[28]
At the social community level, there was a delay in the implementation of restrictive measures. The lockdown started with places of mass gathering, but restaurants and bars were left open for one more week and travel within and outside Italy were not restricted. A total lockdown was imposed in Northern Italy (the “Red Zone“), but not in Central and Southern Italy concurrently; only on March 10, national lockdown was proclaimed. This led to the movement of cases to Southern Italy and subsequently spreading the infection across the entire country.[26] One other fact facilitating the diffusion of the virus and the lack of homogeneity in the national response is that the Italian health system is decentralized and different regions tried varying policy responses. Most notably, Lombardy and Veneto, two neighboring regions with a similar socioeconomic profile and number of cases, tried two different approaches.[26] Veneto tested extensively, both symptomatic and asymptomatic cases, and proactively traced the potential positive cases. If someone tested positive, everyone in the family, as well as neighbors were tested; and if testing kits were unavailable, they were asked to self-quarantine; whenever possible, samples were collected directly from home and processed in the laboratory. In contrast, Lombardy conducted only half of the tests done in Veneto and focused more on symptomatic cases. There was a limited investment in proactive tracing, home care, and monitoring, and protecting healthcare workers. Recently, the epidemic curve flattened, and the number of new cases and deaths stabilized started decreasing only when enormous measures of containment were accomplished. Social media campaigns, movement tracing by the police, and closure of all non-essential activities were finally working; on the other hand, conversion of public places and existing hospitals into intensive care units contributed to the reduction of the fatality rate.
Although the Italian experience might have been a teaching example for the other European countries, a steep increase in the number of cases has been recorded in Spain, France, and the United Kingdom just a few days later. Like Italy, the Spanish government reacted late to the pandemic. On February 19th, 2,500 Valencia soccer fans mingled with 40,000 Atalanta supporters for a Champions League game in Bergamo, which was described as the 'Gamechanger'. A week before the shutdown, on March 8th, several mass events such as sports events, political party activities, conferences, and a massive demonstration for the International Women's Day took place. Three days later, about 3,000 athletic fans flew together for another Champions League match in Liverpool. When the regional government of Madrid closed universities and schools, it provoked a holiday atmosphere, with crowded bars and parks and many people moved to their beach homes.[29] The poor coordination and the delay in implementation of restrictive measures led an abrupt surge of cases in Spain before they enacted the lockdown on March 14, 2020. Only after lockdown, a decline in the number of new cases have been reported [Fig. 3]. We expect a steep decline in new cases in 6-8 weeks provided it is vigorously implemented. To face the burden of the case boom, the government took over all the private healthcare facilities and converted them to COVID-19 care. Due to the shortage of testing kits, laboratory testing was done only for patients needing admission for Severe Acute Respiratory Infections (SARI) and the essential service personnel such as health workers in those departments.[16]
Figure 3.
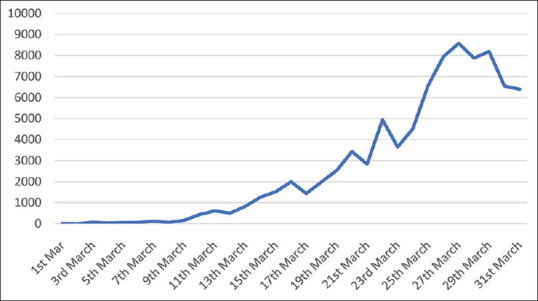
Number of new cases reported from Spain[2]
In the United States (U.S.), there was a lack of coordination in the national response, with an unclear message from the U.S. President with often a variance with information from the U.S. National Institutes of Health (NIH) and the Centers for Disease Control (CDC). Early and severe outbreaks in Washington State and New York State prompted the six counties in the San Francisco Bay Area to impose stay-at-home orders on March 17th, 2020 in response to initial cases. Two days later, the entire state of California was placed under these orders to “flatten the curve“ of new severe cases. The 50 U.S. states and many localities within them individually imposed measures ranging from tight provisions as in California to more lenient approaches such as bans on gatherings and curfews. There was no consistent national policy. This chaotic pattern included a wide variation in travel restrictions and even quarantines for travelers from one state to another and travel restrictions.[30] Even in the absence of enforced restrictions, social distancing was emphasized and those feeling ill were urged to stay home. Early in the epidemic, policy on investigating contacts and quarantining them varied from city to city. For example, in Denver, Colorado, when there were 49 confirmed cases on March 19, health officials reached out to people who might have been exposed only if they were elderly or had underlying health conditions.[31] Health departments in at least two counties in California – Sacramento and Placer counties – decided not to quarantine contacts who did not show symptoms despite growing evidence that asymptomatic carriers might transmit SARS-CoV-2.[31] In Seattle, Washington, the health department was no longer routinely investigating contacts because cases were proliferating rapidly and contact tracing was labor-intensive.[31] There was also an issue with testing due to a shortage of testing kits.[16,32,33] If the country had accurately tracked the spread of the virus, hospitals would have had the opportunity to be prepared and executed their pandemic plans effectively and on time. Suddenly the system was faced with a virus that had been left to spread, untracked, through communities around the country.[34] New York country reported at least 83,712 total positive cases of COVID-19 and more than 1,941 related deaths on April 2nd, 2020, making it the state with the most U.S. coronavirus cases. New York City hospitals were straining under the onslaught of novel coronavirus cases, worsened by a shortage of PPE such as gloves, gowns, and masks and limited availability of ventilators and intensive care beds.[27] This stress on the US healthcare system is likely to increase as cases are projected to peak in some areas during mid-April to late-April and some thereafter. In fact, to track the virus, citizen crowd-sourcing methods have been devised including www.covidnearyou.com, which enables anyone to view the reported health/illness of residents, aggregated by postal zip code.
Among the middle-income countries, Iran was the worst hit. The Iranian government was aware of the outbreak quite early but only little measures were applied to stop it. The connections between Iran and China were not interrupted until January 31st, 2020, in the attempt to maintain strong diplomatic ties.[35] However, the Iranian airlines continued their flights between the two countries up to February 23, 2020.[35] The outbreak was officially acknowledged following only on February 19, 2020, letting the disease spread in the preceding weeks.[35] Iran did not impede the arrangements for the parliamentary elections scheduled on February 21st.[35] Furthermore, it also resisted quarantine measures; the Deputy Health Minister, Iraj Harirchi, publicly opposed it saying “quarantines belong to before World War I for diseases like plague and cholera and even Chinese are not satisfied with the quarantine they had put in place.“[35] Ironically, he later tested positive for coronavirus. In summary, Iran lost multiple opportunities to respond to their worst public health crisis.[35] There were also issues related to a lack of transparency in their reports.[16,36]
A few data on the impact of traveler screening, lockdown, travel restriction, and quarantine is available these days, as the results of these measures have been analyzed only in these days.[37] However, compared to travel restrictions, improved detection, isolation of cases, and social distancing are likely to have a greater impact on the containment of the outbreak. Social distancing also needs to be continued for several months to have a lasting impact. It has been predicted that by reducing the human to human contact by 90%, we can stop the epidemic.[38] Countries that have implemented social distancing earlier had a greater doubling time (South Korea, Singapore, Japan, Hong Kong) as compared to countries that did not (US, France, Italy).[39] The use of face masks by everyone is still controversial, though WHO does not recommend use by everyone, other agencies do recommend it.[40,41]
India's Response to COVID-19
In India, the first case of COVID-19 was reported on January 30th, 2020, followed by two similar cases on February 2nd and 3rd. All three had a travel history to Wuhan, China. A month later, on March 2nd, two new cases were reported – one each from New Delhi and Hyderabad. A sharp increase in numbers then followed.
To contain the spread, the Ministry of Health and Family Welfare (MoHFW) immediately took action and issued a travel advisory, as travel restrictions had previously demonstrated efficacious on outbreaks of SARS, Ebola, and bubonic plague. All international travelers entering the country were asked to self-quarantine for 14 days. All travel visas to other countries were canceled until April 15th, 2020. All the states were asked to invoke the Epidemic Disease Act, which allowed officials to quarantine suspected cases and close down public places. An intensive campaign was rolled out and guidelines were developed for personal hygiene, surveillance, contact tracing, quarantine, diagnosis, laboratory tests, and management. People were advised not to visit farms, live animal markets or places where animals are slaughtered and to avoid mass gatherings. All the health care facilities were asked to stop regular out-patient and in-patient services and to continue with solely emergency services. Doctors were encouraged to use telemedicine services. Arogya Setu app was also launched to connect essential health services with people of India to fight against COVID-19. This app will reach out and inform the users of the risk, best practice and relevant advisories pertaining to containment of COVID-19. Amenities like hotels, colleges, railway train coaches, etc., were converted into quarantine facilities and large public places as stadiums were converted into isolation wards to handle an anticipated increased number of cases. Some of the states converted existing hospitals to exclusively handle COVID-19 patients. On March 22nd, Prime Minister Narendra Modi initiated the lockdown process with a 14-hour 'Janta Curfew', followed by lockdown in 75 COVID-19 affected districts and a nationwide lockdown for the 3 weeks. A containment plan involving the State and twenty ministries was set up. A round-the-clock control room was set up at the headquarters of the General Director of Health Service (DGHS) to address the virus-related queries. The countries of the South Asian Association for Regional Cooperation (SAARC) were invited to fight jointly against this pandemic and 10 million US dollars were allocated for SAARC countries. A huge evacuation program of many Indian nationals was done from the COVID-19 affected areas.
All the measures implemented in India are revealing efficiency in flattening the curve. Nevertheless, a small effort has been addressed to the identification of asymptomatic and mild cases. This might have detrimental effects on the Indian economy in the long term. A long duration of the lockdown might be more devastating in India than in wealthier countries like the United Kingdom or Australia, and it could result in serious economic damage, increased hunger, and poverty, and it might reduce the population's resilience to handle the infection. Therefore, if these cases remain unidentified, there is a possibility of another peak of COVID-19 cases once the lockdown is lifted, and India's healthcare system might be not able to handle it properly. Hence, moving ahead, India should have 'staggered' exit from the lockdown, especially in the COVID-19 hotspot areas and use this lockdown period to screen and identify as many cases as possible, isolate them and quarantine their contacts. As compared to other countries worldwide, a very low number of tests have been run in India [Fig. 4], with the highest number done in Kerala [Table 1]; testing is done in 122 government labs and 44 private laboratories, however it is likely to increase in the near future.[42] At the time this article is being written, 158 districts in India have recorded at least one COVID-19 case.[42] Hence, this opportunity should be taken to screen the high-risk areas in these districts using the mid-level personnel, both from the government and private sectors. At the same time, the capacity for rapid diagnostic testing at the primary level should be implemented, to identify cases earlier and limit the transmission. This period should be also utilized for producing a large supply of PPE for the safety of health care workers and increasing the number of available ventilators, in case the outbreak worsens.
Figure 4.
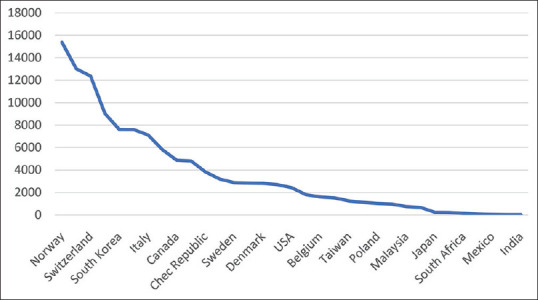
Test done for COVID-19 per million population in different countries (as on 29th March)[39]
Table 1.
Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) test done in India (as on 27th March).[39]
| State | Tests done | Total positive cases |
|---|---|---|
| Kerala | 5432 | 182 |
| Karnataka | 3076 | 76 |
| Rajasthan | 2325 | 55 |
| Tamil Nadu | 1500 | 49 |
| Telangana | 1319 | 66 |
| Haryana | 1003 | 33 |
| Andhra Pradesh | 496 | 19 |
| West Bengal | 389 | 18 |
| Jammu and Kashmir | 379 | 31 |
| Chhattisgarh | 376 | 7 |
| Odisha | 297 | 3 |
| Madhya Pradesh | 251 | 47 |
In conclusion, India and the world have a long legacy of successful efforts to prevent or cure widespread infections. Recalling the successful smallpox eradication campaign of the 1970s, we are reminded of the pivotal role of leadership and sound management to stop the killer disease.[43] Hence, India has the opportunity to reverse disease predictions with stringent containment measures, social distancing, increasing case detection, isolation and quarantining the contacts. Efforts should be made to enlist community support and ownership so containment measures do not depend exclusively on administrative measures; critical situations like a mass exodus of laborers from the major cities to the rural areas as well as mass gatherings like Nizamuddin Markaz event which happened recently should be avoided.
Global Impact of COVID-19
As the impact of COVID-19 is not limited to human infection and death, other associated issues should be addressed, like social discrimination. For instance, healthcare workers are increasingly looked at as someone who can spread the virus in the community. Furthermore, Asian Americans have been experiencing a rising number of episodes of violence and hate after U.S. President made hurtful and misleading comments as “China is to blame“ and calling COVID-19 the “Chinese virus.“
The impact of COVID has been also affecting sectors like entertainment, tourism, restaurants, and the travel industry, with a tremendous escalation of job losses.[44] Disrupted supply chain and declining stock markets are the final consequences of these social changes, thus hitting the global economy.[44] Finally, a greater incidence of panic disorder, anxiety, depression, and other psychosocial issues has been reported.[45]
Future Directions
Looking into the near future, containing the COVID-19 epidemic is likely to take several months; public health interventions will be directed towards social distancing and improving hygienic practices. These interventions will be effective in delaying the onset of wide community transmission, reducing peak incidence and its impact on public services.[5] Testing, contact tracing, isolation of infected, and precautionary self-isolation of contacts is critical in reducing the number of new cases.[46] An exceptionally high degree of understanding in the population and acceptance of these measures is also critical.[46] These interventions have to be balanced with getting back to normal life and everyday activities to the best extent possible until a reversing the trajectory of the pandemic is traced.[47]
A little knowledge is available so far on alternate routes of transmission, namely via sewage, contaminated water, or air conditioning systems. It is also poorly known if those who have recovered from SARS-CoV-2 infection would be protected from reinfection, but evidence to confirm this is yet to be generated. Antibody testing has to be implemented on a large scale to identify who is already immune to the virus. The effect of temperature, season, and humidity on COVID-19 also has an impact on the COVID-19 outbreak, however, results from other parts of the world are awaited.[48,49]
Multiple trials are currently underway to develop novel treatment options as well as a vaccine to treat the respiratory syndrome, but results are still awaited.[50] Moreover, months are needed before a vaccine is developed and approved. Even though herd immunity develops over time, vulnerable groups as the healthcare workforce and elderly people should still be preserved. Smart working and staggered shifts may have to be adopted to mitigate COVID-19 transmission in the future. Digital didactic and online learning can be protracted for months. Telemedicine, and in particular teleophthalmology, needs to be implemented. Also in the future, infectious diseases will be probably included amongst the most important health hazards along with anti-microbial resistance.[51] In addition, timely identification, efficient diagnosis, rapid isolation, and clinical management would remain in the forefront.[51]
One of the last concerns regards the second wave of COVID-19 outbreak. Asian countries and cities that seemed to have brought the coronavirus epidemic under control are suddenly tightening their borders and imposing stricter containment measures, fearful about new imported infections. Hong Kong suddenly saw new cases spike as high as 65 in one day and ordered a new closure of non-essential activities. In Japan, where infections have remained relatively controlled, cases started to rise in March as travelers returned in the home country. New cases of local transmission have also been detected. Similarly, Singapore again announced one-month lockdown in view of increased local transmission. This portends a worrisome sign for the United States, Europe, India and the rest of the world regarding the second wave of the virus spreading once the restrictive measures are relieved.[52]
Conclusion
Over the past two months, COVID-19 has emerged as a public health threat around the world. It adds to the list of previous epidemic infectious disease outbreaks, including Bovine Spongiform Encephalitis in 1986, the Avian flu in 1997, the SARS in 2002, the Swine Flu in 2009, and the Ebola in 2014. All these outbreaks remind us that we live in a habitat where it is necessary to respect the relationship between animal, social life, and the environment to survive and thrive. Rapid urbanization and our incursion into forest lands, has created a new interface between humans and wildlife; and exposed humans to unfamiliar organisms often involving the consumption of exotic wildlife. As stated by the UN Environment Chief, Inger Anderson “Our continued erosion of wild space has brought us uncomfortably close to animal and plants that harbor diseases that can jump to humans.“ She said, “If we don't take care of nature, we can't take care of ourselves“.[53] With COVID-19, nature is sending us a message that we need to recognize the interrelationship between animals, including pets, livestock and wildlife. The transdisciplinary OneHealth approach involving professionals from many disciplines such as medicine, veterinary, environmental health, and social sciences has been advocated to limit new infectious outbreaks.[54] The global experience is teaching that containment measures and aggressive contract tracing are mandatory to keep the infection under control until an approved treatment or a vaccine is available to the global community. They should also minimize the economic burden of disease, and improve understanding of disease mechanisms, health problems, disease emergence, and reemergence to respond in a proportionate and timely manner. This will help in detecting, preventing, and combating future pandemics based on our experience from COVID-19 outbreaks. The implementation and development of the OneHealth collaborations on a global scale are critical in reducing the threat of emerging viruses.[54]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
We would like to acknowledge the following members for their contribution to the manuscript: Dr. Manoj V. Murhekar, Director and Scientist, National Institute of Epidemiology, Indian Council of Medical Research, Chennai, Tamil Nadu and Dr Larry Brilliant, Chair, Ending Pandemics; Founder Seva Foundation and CEO, Pandefense and CNN on-air analyst. Dr Brilliant is an alumnus of the WHO Smallpox Eradication program. We would also like to acknowledge Ms Sreedevi Penmetcha, Management consultant at L V Prasad Eye Institute for language editing of the manuscript.
References
- 1.Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet (London, England) 2020;395:470–3. doi: 10.1016/S0140-6736(20)30185-9. doi: 10.1016/s0140-6736 (20) 30185-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. [Last accessed on 2020 Mar 31]. Available from: https://www.who.int/emergencies/diseases/novel- coronavirus-2019 .
- 3.Mahase E. Coronavirus covid-19 has killed more people than SARS and MERS combined, despite lower case fatality rate. BMJ (Clinical research ed) 2020;368:m641. doi: 10.1136/bmj.m641. doi: 10.1136/bmj. [DOI] [PubMed] [Google Scholar]
- 4.Chan-Yeung M, Xu RH. SARS: Epidemiology. Respirology (Carlton, Vic) 2003;8(Suppl):S9–14. doi: 10.1046/j.1440-1843.2003.00518.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wilder-Smith A, Chiew CJ, Lee VJ. Can we contain the COVID-19 outbreak with the same measures as for SARS. The Lancet Infectious diseases. 2020 doi: 10.1016/S1473-3099(20)30129-8. doi: 101016/s1473-3099 (20) 30129-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wilder-Smith A, Teleman MD, Heng BH, Earnest A, Ling AE, Leo YS. Asymptomatic SARS coronavirus infection among healthcare workers, Singapore. Emerg Infect Dis. 2005;11:1142–5. doi: 10.3201/eid1107.041165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med. 2020;382:970–1. doi: 10.1056/NEJMc2001468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Quilty BJ, Clifford S, Flasche S, Eggo RM. Effectiveness of airport screening at detecting travellers infected with novel coronavirus (2019-nCoV) Euro Surveillance. 2020:25. doi: 10.2807/1560-7917.ES.2020.25.5.2000080. doi: 102807/1560-7917 Es 20202552000080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Anderson RM, Heesterbeek H, Klinkenberg D, Hollingsworth TD. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet (London, England) 2020;395:931–4. doi: 10.1016/S0140-6736(20)30567-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J Hosp Infect. 2020;104:246–51. doi: 10.1016/j.jhin.2020.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020 doi: 10.1056/NEJMc2004973. doi: 101056/NEJMc2004973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Prem K, Liu Y, Russell TW, Kucharski AJ, Eggo RM, Davies N, et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health. 2020 doi: 10.1016/S2468-2667(20)30073-6. doi: 101016/s2468-2667 (20) 30073-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. [Last accessed on 2020 Mar 31]. Available from: https://www.worldpop.org/events/COVID_NPI .
- 14.Bogoch II, Watts A, Thomas-Bachli A, Huber C, Kraemer MUG, Khan K. Potential for global spread of a novel coronavirus from China. J Travel Med. 2020:27. doi: 10.1093/jtm/taaa011. doi: 101093/jtm/taaa011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bogoch, Watts A, Thomas-Bachli A, Huber C, Kraemer MUG, Khan K. Pneumonia of unknown aetiology in Wuhan, China: Potential for international spread via commercial air travel. J Travel Med. 2020:27. doi: 10.1093/jtm/taaa008. doi: 101093/jtm/taaa008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tanne JH, Hayasaki E, Zastrow M, Pulla P, Smith P, Rada AG. COVID-19: How doctors and healthcare systems are tackling coronavirus worldwide. BMJ. 2020;368:m1090. doi: 10.1136/bmj.m1090. [DOI] [PubMed] [Google Scholar]
- 17.Lau H, Khosrawipour V, Kocbach P, Mikolajczyk A, Schubert J, Bania J, et al. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J Travel Med. 2020 doi: 10.1093/jtm/taaa037. doi: 101093/jtm/taaa037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cyranoski D. What China's coronavirus response can teach the rest of the world. Nature. 2020;579:479–80. doi: 10.1038/d41586-020-00741-x. [DOI] [PubMed] [Google Scholar]
- 19.Chen W, Wang Q, Li YQ, Yu HL, Xia YY, Zhang ML, et al. Early containment strategies and core measures for prevention and control of novel coronavirus pneumonia in China. Zhonghua Yu Fang Yi Xue Za Zhi [Chinese J Prev Med] 2020;54:1–6. doi: 10.3760/cma.j.issn.0253-9624.2020.03.003. [DOI] [PubMed] [Google Scholar]
- 20.Kucharski AJ, Russell TW, Diamond C, Liu Y, Edmunds J, Funk S, et al. Early dynamics of transmission and control of COVID-19: A mathematical modelling study. Lancet. 2020 doi: 10.1016/S1473-3099(20)30144-4. doi: 101016/S1473-3099 (20) 30144-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tian H, Liu Y, Li Y, Wu C, Chen B, Kraemer MUG, et al. The impact of transmission control measures during the first 50 days of the COVID-19 epidemic in China. medRxiv. 2020 doi: 10.1126/science.abb6105. doi: 101101/2020013020019844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chinazzi M, Davis JT, Ajelli M, Gioannini C, Litvinova M, Merler S, et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science. 2020 doi: 10.1126/science.aba9757. doi: 101126/scienceaba9757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wong JEL, Leo YS, Tan CC. COVID-19 in Singapore-current experience: Critical global issues that require attention and action. JAMA. 2020 doi: 10.1001/jama.2020.2467. doi: 101001/jama 20202467. [DOI] [PubMed] [Google Scholar]
- 24.Lee VJ, Chiew CJ, Khong WX. Interrupting transmission of COVID-19: Lessons from containment efforts in Singapore. J Travel Med. 2020 doi: 10.1093/jtm/taaa039. doi: 101093/jtm/taaa039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. [Last accessed on 2020 Mar 31]. Available from: https://www.gov.sg/article/what-do-the-differentdorscon-levels-mean .
- 26. [Last accessed on Mar 31]. Available from: https://hbr.org/2020/03/lessons-from-italysresponse-to-coronavirus .
- 27.Emanuel EJ, Persad G, Upshur R, Thome B, Parker M, Glickman A, et al. Fair allocation of scarce medical resources in the time of COVID-19. N Engl J Med. 2020 doi: 10.1056/NEJMsb2005114. doi: 101056/NEJMsb2005114. [DOI] [PubMed] [Google Scholar]
- 28.Paterlini M. On the front lines of coronavirus: The Italian response to covid-19. BMJ (Clinical research ed) 2020;368:m1065. doi: 10.1136/bmj.m1065. [DOI] [PubMed] [Google Scholar]
- 29. [Last accessed on 2020 Mar 31]. Available from: https://www.theguardian.com/world/2020/mar/26/spain- coronavirus-response-analysis .
- 30.Gostin L, Wiley L. Governmental public health powers during the COVID-19 pandemic: Stay-at-home orders, business closures, and travel restrictions. JAMA. 2020 doi: 10.1001/jama.2020.5460. doi: 101001/jama 20205460. [DOI] [PubMed] [Google Scholar]
- 31. [Last accessed on 2020 Mar 31]. Available from : https://www.nature.com/articles/d41586-020-00823-w .
- 32.Gostin LO, Hodge JG, Jr US emergency legal responses to novel coronavirus: Balancing public health and civil liberties. JAMA. 2020;323:1131–2. doi: 10.1001/jama.2020.2025. [DOI] [PubMed] [Google Scholar]
- 33.Gostin LO, Hodge JG., Jr US emergency legal responses to novel coronavirus: Balancing public health and civil liberties. JAMA. 2020;323:1131–2. doi: 10.1001/jama.2020.2025. [DOI] [PubMed] [Google Scholar]
- 34.Haffajee RL, Mello MM. Thinking globally, acting locally — The US response to COVID-19. N Engl J Med. 2020 doi: 10.1056/NEJMp2006740. doi: 101056/NEJMp2006740. [DOI] [PubMed] [Google Scholar]
- 35. [Last accessed on 2020 Mar 31]. Available from: https://foreignpolicy.com/2020/03/24/how-iran-botched- coronavirus-pandemic-response/
- 36.Abdi M. Coronavirus disease 2019 (COVID-19) outbreak in Iran; actions and problems? Infect Control Hosp Epidemiol. 2020:1–5. doi: 10.1017/ice.2020.86. doi: 10.1017/ice. 2020.86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wells CR, Sah P, Moghadas SM, Pandey A, Shoukat A, Wang Y, et al. Impact of international travel and border control measures on the global spread of the novel 2019 coronavirus outbreak. Proc Natl Acad Sci U S A. 2020;117:7504–9. doi: 10.1073/pnas.2002616117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Hellewell J, Abbott S, Gimma A, Bosse NI, Jarvis CI, Russell TW, et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Global Health. 2020;8:e488–e96. doi: 10.1016/S2214-109X(20)30074-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. [Last accessed on 2020 Mar 31]. Available from : https://factly.in/covid-19-testing-who-is-testing-how-many/
- 40. [Last accessed on Mar 31]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting- sick/cloth-face-cover.html#studies .
- 41.Feng S, Shen C, Xia N, Song W, Fan M, Cowling BJ. Rational use of face masks in the COVID-19 pandemic. Lancet Respir Med. 2020 doi: 10.1016/S2213-2600(20)30134-X. doi: 101016/s2213-2600 (20) 30134-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. [Last accessed on 2020 Mar 8]. Available from: https://www.mohfw.gov.in/
- 43.Brilliant, Lawrence B. The Management of Smallpox Eradication in India University of Michigan Press. Ann Arbor. 1985 [Google Scholar]
- 44.Shah SGS, Farrow A. A commentary on “World Health Organization declares global emergency: A review of the 2019 novel Coronavirus (COVID-19)“. Int J Surg (London, England) 2020;76:128–9. doi: 10.1016/j.ijsu.2020.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen Psychiatr. 2020;33:e100213. doi: 10.1136/gpsych-2020-100213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Salathe M, Althaus CL, Neher R, Stringhini S, Hodcroft E, Fellay J, et al. COVID-19 epidemic in Switzerland: On the importance of testing, contact tracing and isolation. Swiss Med Wkly. 2020;150:w20225. doi: 10.4414/smw.2020.20225. [DOI] [PubMed] [Google Scholar]
- 47.Yuen KS, Ye ZW, Fung SY, Chan CP, Jin DY. SARS-CoV-2 and COVID-19: The most important research questions. Cell Biosci. 2020;10:40. doi: 10.1186/s13578-020-00404-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Chan KH, Peiris JS, Lam SY, Poon LL, Yuen KY, Seto WH. The effects of temperature and relative humidity on the viability of the SARS coronavirus. Adv Virol. 2011;2011:734690. doi: 10.1155/2011/734690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Shi P, Dong Y, Yan H, Li X, Zhao C, Liu W, et al. The impact of temperature and absolute humidity on the coronavirus disease 2019 (COVID-19) outbreak-evidence from China. medRxiv. 2020 doi: 101101/2020032220038919. [Google Scholar]
- 50.Zhou M, Zhang X, Qu J. Coronavirus disease 2019 (COVID-19): A clinical update. Front Med. 2020 doi: 10.1007/s11684-020-0767-8. Epub 2020/04/03 doi: 101007/s11684-020-0767-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Mattiuzzi C, Lippi G. Which lessons shall we learn from the 2019 novel coronavirus outbreak? Ann Transl Med. 2020;8:48. doi: 10.21037/atm.2020.02.06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Cyranoski D. 'We need to be alert': Scientists fear second coronavirus wave as China's lockdowns ease. Nature. 2020 doi: 10.1038/d41586-020-00938-0. doi: 101038/d41586-020-00938-0. [DOI] [PubMed] [Google Scholar]
- 53. [Last accessed on 2020 Mar 31]. Available from: https://www.theguardian.com/world/2020/mar/25/coronavirus-nature-is-sending-us-a-message-says-unenvironment-chief .
- 54.Kelly TR, Karesh WB, Johnson CK, Gilardi KV, Anthony SJ, Goldstein T, et al. One health proof of concept: Bringing a transdisciplinary approach to surveillance for zoonotic viruses at the human-wild animal interface. Prev Vet Med. 2017;137:112–8. doi: 10.1016/j.prevetmed.2016.11.023. doi: 10.1016/j.prevetmed. 2016.11.023. [DOI] [PMC free article] [PubMed] [Google Scholar]