
Figure 3.
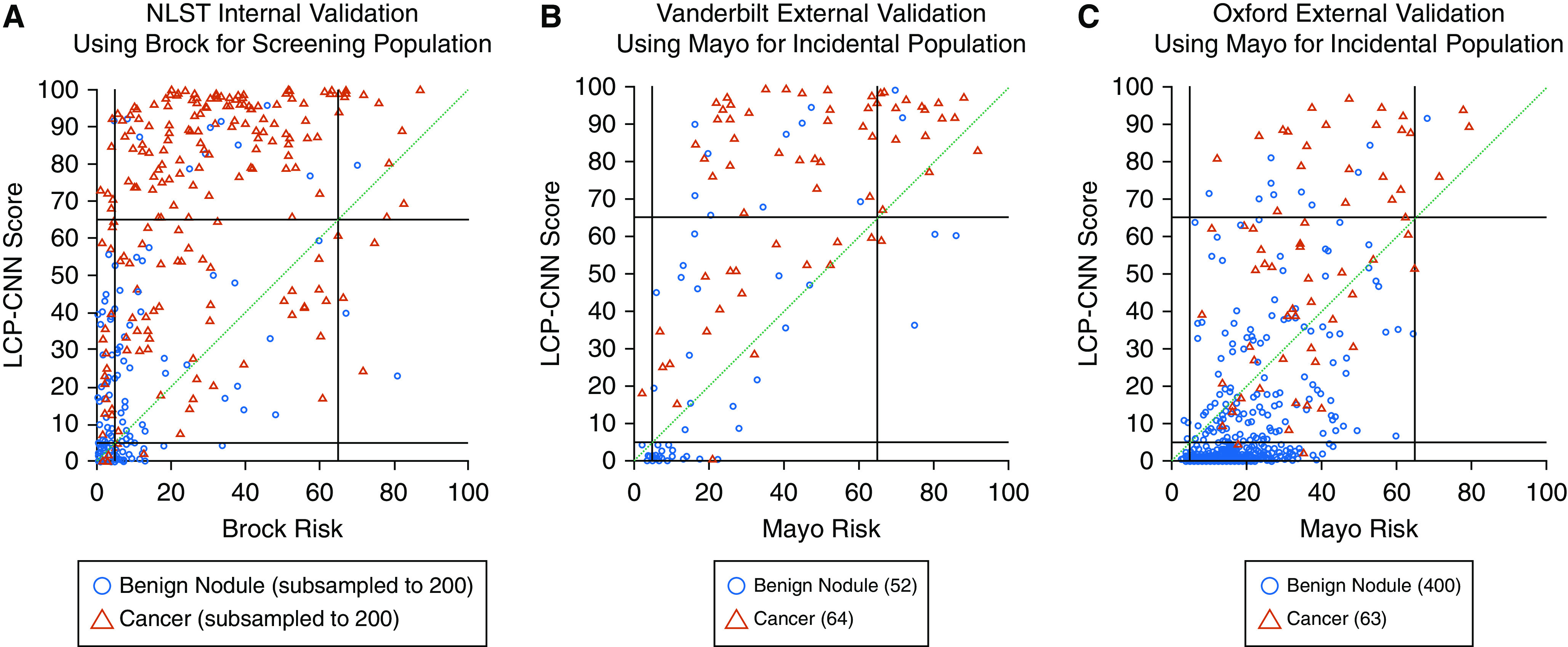
Reclassification diagrams. (A) National Lung Screening Trial (NLST) dataset for 200 cases and 200 benign nodules (randomly selected; numbers were limited for readability of the figure). (B) Vanderbilt University Medical Center dataset. (C) Oxford University Hospitals dataset. Reclassification diagrams are a useful way to visualize the impact of a new biomarker compared with a reference at predefined thresholds. Here we use rule-out and rule-in thresholds at 5% and 65%, respectively, as shown by the black lines. Red triangles indicate cancers, and blue circles indicate controls. If a new biomarker improves classification of cancers compared with the reference, then one would expect, for example, cases (red triangles) that were below 65% on the horizontal axis to move above 65% to the vertical axis, that is, from the central rectangular region to the region immediately above it. For example, on the Vanderbilt and Oxford datasets, 45% and 32% of the cancers, respectively, are reclassified up compared with the Mayo model. Similarly, a new biomarker improves benign classification compared with the reference if it moves controls (blue circles) that were above the 5% threshold on the horizontal axis to below 5% on the vertical axis. For nodules that stay within the three square regions intersected by the green diagonal, the Lung Cancer Prediction Convolutional Neural Network (LCP-CNN) does not add value because none of the nodules are correctly reclassified compared with the Brock or Mayo model. On the Vanderbilt and Oxford datasets, 33% and 61% of the benign nodules, respectively, are reclassified down compared with the Mayo model.