
Figure 8.
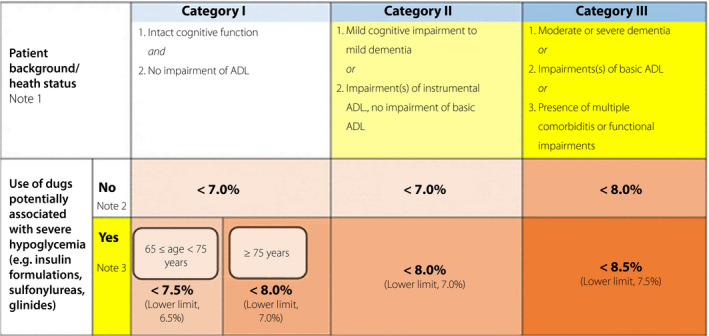
Glycemic control targets (HbA1c values) for elderly patients with diabetes. The glycemic target is to be determined for each patient by taking into account his/her age, duration of diabetes, risk for hypoglycemia, and any support available to the patient, as well as the patient’s cognitive function, basic/instrumental ADL, and comorbidities/functional impairments, while noting the potential risk of hypoglycemia that increases with age in each patient. Note 1: Refer to the Japan Geriatrics Society website (https://www.jpn‐geriat‐soc.or.jp/tool/index.html), for the evaluation of the cognitive function, basic ADL (e.g. self‐care abilities such as dressing, mobility, bathing, and toileting), and instrumental ADL (e.g. abilities to maintain an independent household such as shopping, meal preparation, taking medication, and handling finances). In end‐of‐life care, priority is to be given to preventing significant hyperglycemia and subsequent dehydration and acute complications through appropriate therapeutic measures. Note 2: As in other age groups, the glycemic target is set at <7.0% in the elderly for preventing diabetic complications. However, this could be set at <6.0% for those likely to achieve glycemic control through diet and exercise therapy alone or those likely to achieve glycemic control with drug therapy without adverse reactions, or 8.0% for those in whom intensifying therapy may prove difficult. In either case, no lower limit is specified for the glycemic target. A glycemic target of <8.5% may be allowed in patients thought to be in category III and therefore at risk of developing adverse reactions to multi‐drug combination therapy or in those with serious comorbidities or poor social support. Note 3: In patients in whom priority should be given to preventing the onset/progression of diabetic complications due to their duration of disease, the glycemic control target or its lower limit may be set for each elderly patient with appropriate measures in order to prevent severe hypoglycemia. In patients in whom any of these agents was initiated before the age of 65 and whose HbA1c values are shown to fall below their glycemic control targets described above, current treatments are to be continued, with utmost care being taken to avoid potential severe hypoglycemia. Glinides may be classified as drugs unlikely to be associated with severe hypoglycemia, as the onset of severe hypoglycemia varies depending on the type and amount of glinide used in a particular patient relative to the patient’s glucose level. (Cited from Haneda, M., Inagaki, N., Suzuki, R. et al. Glycemic targets for elderly patients with diabetes. Diabetol Int 7, 331–333 (2016). https://doi.org/10.1007/s13340‐016‐0293‐8).