
Figure 3.
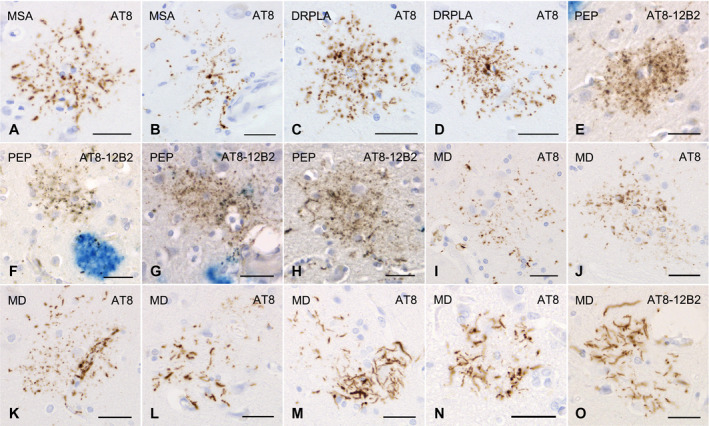
GFAs and other distinctive tau‐positive astrocytic lesions in cases of multiple system atrophy, dentatorubral‐pallidoluysian atrophy, postencephalic parkinsonism and myotonic dystrophy. A, B. GFAs in an MSA case with PART but without any other primary tauopathy. AT8 immunohistochemistry. The amygdala. C, D. GFAs in a DRPLA case with PART but without any other primary tauopathy. AT8 immunohistochemistry. The amygdala. E–H. Double immunohistochemistry for tau (AT8, brown) and Aβ (12B2, blue) of GFA‐like astrocytic tau pathologies in a case of postencephalitic parkinsonism. Glial lesions that are composed of fine tau‐positive granules are usually independent of Aβ deposits. The amygdala. I–O. GFAs and distinct tau‐positive astrocytic lesions in cases of myotonic dystrophy (MD). AT8 immunohistochemistry. I–K. GFAs in an MD case. The amygdala. Some GFAs were in contact with vessel walls, in which tau was densely accumulated in astrocytic endfeet touching the vessel (K). L. Tau‐positive astrocytic lesions having both twisted or crinkly thin threads and granular components like those observed in GFAs in an MD case. The frontal cortex. M, N. Tau‐positive astrocytic lesions that include almost only twisted or crinkly thin threads in an MD case. The frontal cortex. O. Astrocytic lesions mainly composing of longer twisted tau‐positive threads in addition to various quantities of fine tau‐positive granules are often noted in an MD case. Twisted fine threads are often radially arranged, appearing to be reminiscent of threads in astrocytic plaques in CBD. However, the threads of astrocytic lesions in MD cases tend to be finer and longer than those usually observed in astrocytic plaques in CBD cases (see Figure 2O). The frontal cortex. All scale bars = 30 μm.