
2. Proposed central role of LDL, PCSK9, LDLR and CD36 in modulating the risk for CVD vs. T2D.
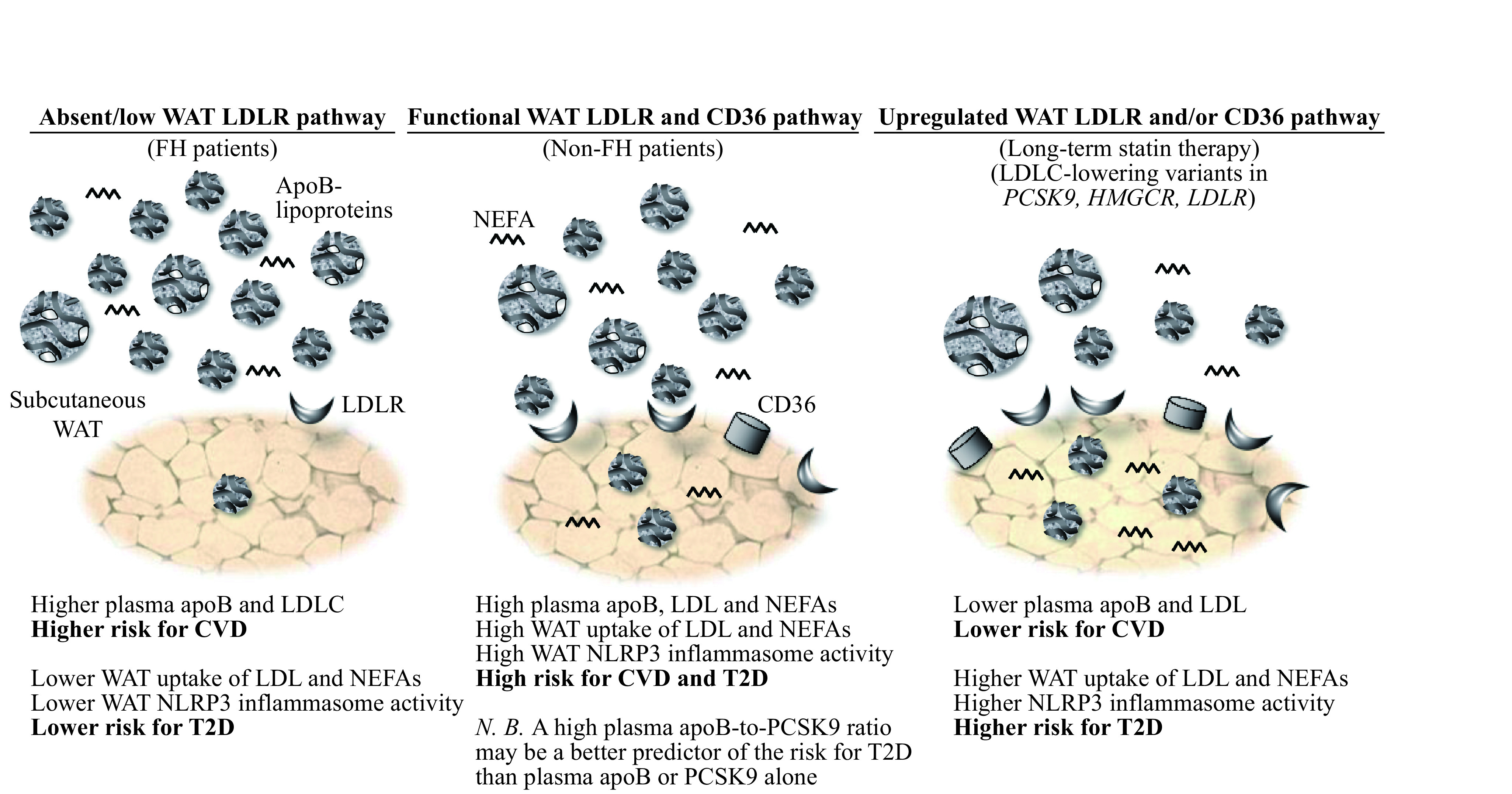
Patients with familial hypercholesterolemia with marked reduction or absence of a functional LDLR pathway have higher risk for CVD but lower risk for T2D despite very high plasma LDL. Conversely, patients with induced (statin therapy) or inherited (LDLC-lowering variants in PCSK9, HMGCR and LDLR) upregulated LDLR pathway have lower risk for CVD but higher risk for T2D despite low plasma LDL and apoB (N.B. CD36 pathway may also be upregulated in subjects with PCSK9 LOF variants). In between these 2 extremities in non-FH patients, the higher plasma apoB, mostly as LDL, the higher is the risk for both CVD and T2D. A higher plasma apoB-to-PCSK9 ratio may indicate a higher risk for T2D than plasma apoB alone as it may predict upregulated WAT surface-expression of LDLR and CD36 and receptor-mediated LDL uptake. WAT: white adipose tissue; FH: familial hypercholesterolemia; LDL: low-density lipoprotein; LDLR: LDL receptor; NEFAs: non-esterified fatty acids; PCSK9: proprotein convertase subtilisin/kexin type 9; CD36: cluster of differentiation 36; HMGCR: 3-hydroxy-3-methylglutaryl-coenzyme A reductase; NLRP3: nucleotide-binding domain and Leucine-rich repeat receptor, containing a Pyrin domain 3; T2D: type 2 diabetes; CVD: cardiovascular disease.