
Figure 2. Pathogenesis of LTBI and its reactivation upon HIV co-infection.
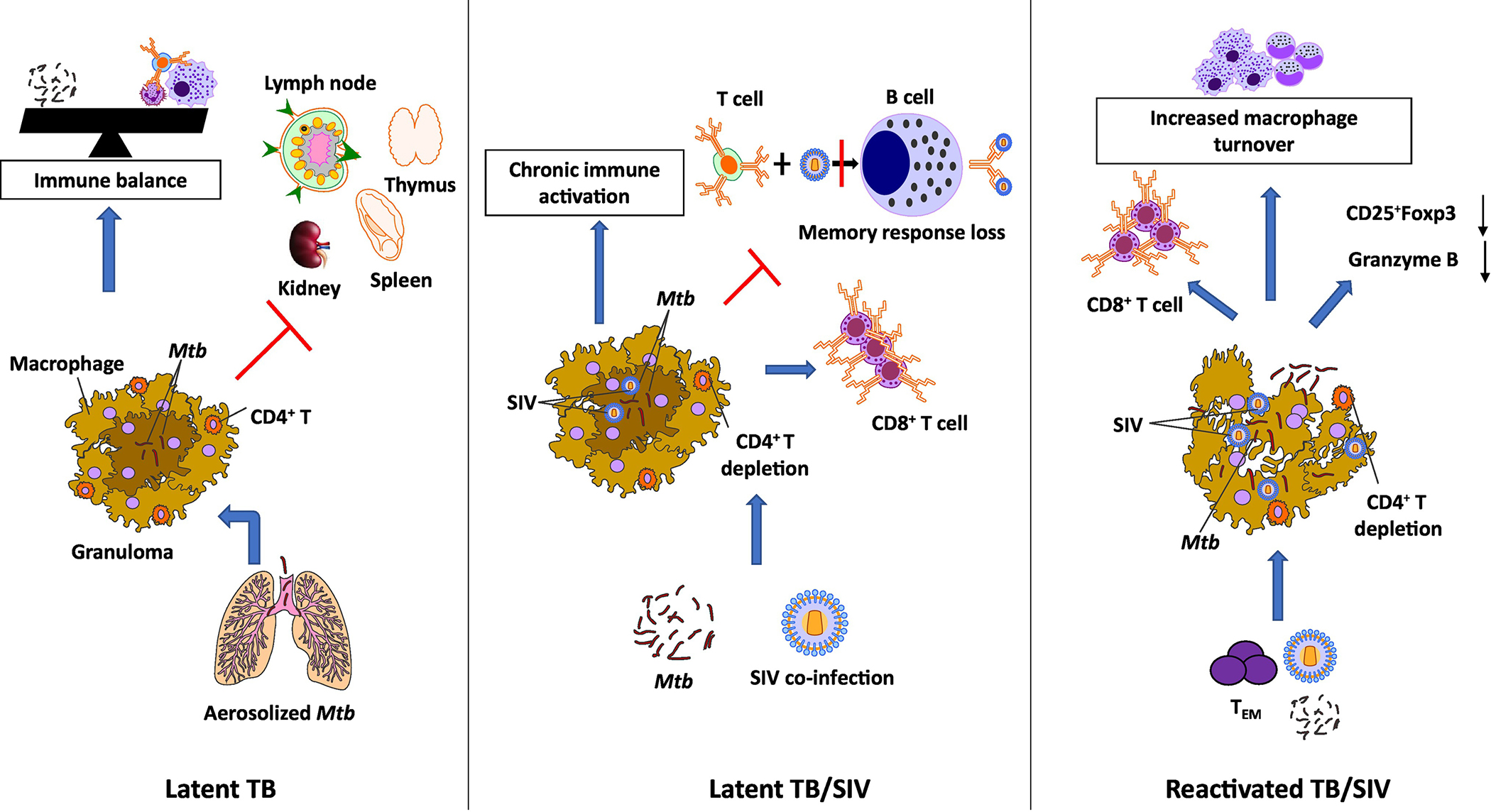
LTBI is characterized by a dynamic balance between the pathogen and the host as a consequence of limited bacterial replication due to its containment within granulomas. Inhaled droplet Mtb nuclei are engulfed by the macrophages and dendritic cells in the terminal alveoli in the lungs. In the latent phase, the replication is contained with the granuloma by the activated T lymphocytes and macrophages. This leads to an arrest of the disease progression and an immune balance is attained. Co-infection with SIV leads to a severe immunosuppression and a drastic decrease in CD4+ T cell counts in the granulomas. As a result, there is an increase in the number of CD8+ T cells with increased expression of activation markers, CD95, CD38 and HLA-DR. A reduced expression of CD25 on B cells during SIV infection results in perturbation of the B cell response to CD4+ T cells. A reduced antigen presentation from CD4+ T cells impairs the generation of memory B cells. Taken together, SIV co-infection of Mtb leads to chronic immune activation, immune dysbiosis and a skewed Treg/TH17 balance resulting in reactivation of LTBI. Following the SIV-induced immune perturbation, there is a reduction in the generation of lung homing Mtb-specific TEM CD4+ T cells. This preferred depletion of Mtb-specific CD4+ T cells and viral infection of the macrophages in the granulomas causes the integrity of the granuloma to disintegrate leaking the contained Mtb leading to dissemination.