
Fig. 5.
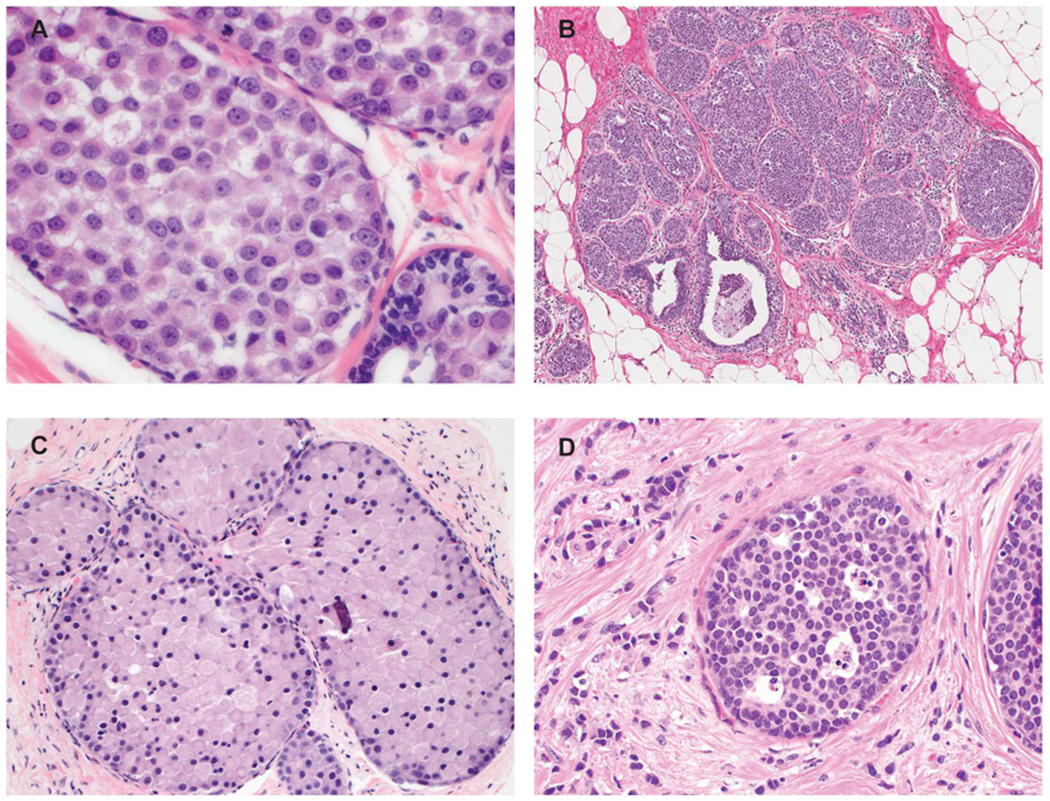
Borderline and unusual LCIS lesions. A. In this LCIS case, the nuclei are larger than those of typical type B cells but fall short of the marked atypia required for pleomorphic LCIS. The lesion should be categorized as classic LCIS composed of type B cells. B. This LCIS lesion shows abundant proliferation with significantly expanded acini. However, the acini remain separate from one another with persistence of intervening interlobular stroma and none of the distended acini fill one high power field. The lesion does not meet the criteria for florid LCIS and should be classified as classic LCIS. C. This example of LCIS with apocrine features but lacking marked nuclear pleomorphism is challenging to classify. It should not be diagnosed as apocrine pleomorphic LCIS or simply “non-classic LCIS”. One suggested approach is to give the descriptive diagnosis “LCIS with apocrine features” with a comment in the report. D. This LCIS lesion is composed of classic lobular cells (type A) but shows single-cell apoptosis and minute foci of necrosis. In the absence of marked nuclear atypia or duct-lobular expansion, the lesion is best classified as classic LCIS.