
FIGURE 2.
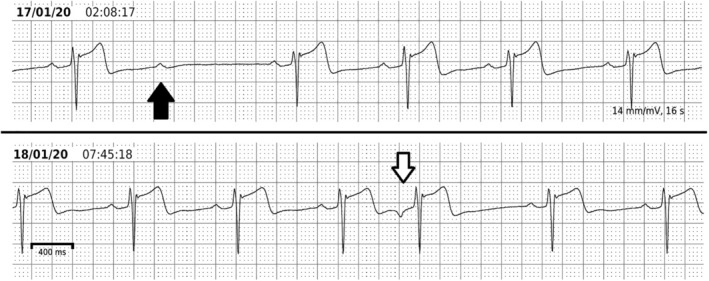
Ambulatory ECG findings that rule out pre‐excitation. This athlete was investigated because of a relatively short PR interval (115 ms) with non‐specific broadening of the QRS complex on a routine 12‐lead ECG. A 5‐day, single derivation recording was performed. This shows lengthening of the PR interval to 200 ms during sleep without alteration of the QRS complex. There are also instances of second degree AV block during sleep (black arrow) and atrial premature beats which are conducted at a longer PR interval without alteration in the QRS complex. All of these features indicate that either the patient has no pathway capable of anterograde conduction or that the AERP of the pathway is longer than the sinus cycle present at the time of the second degree AV block, which was over 1 s