
Fig. 3.
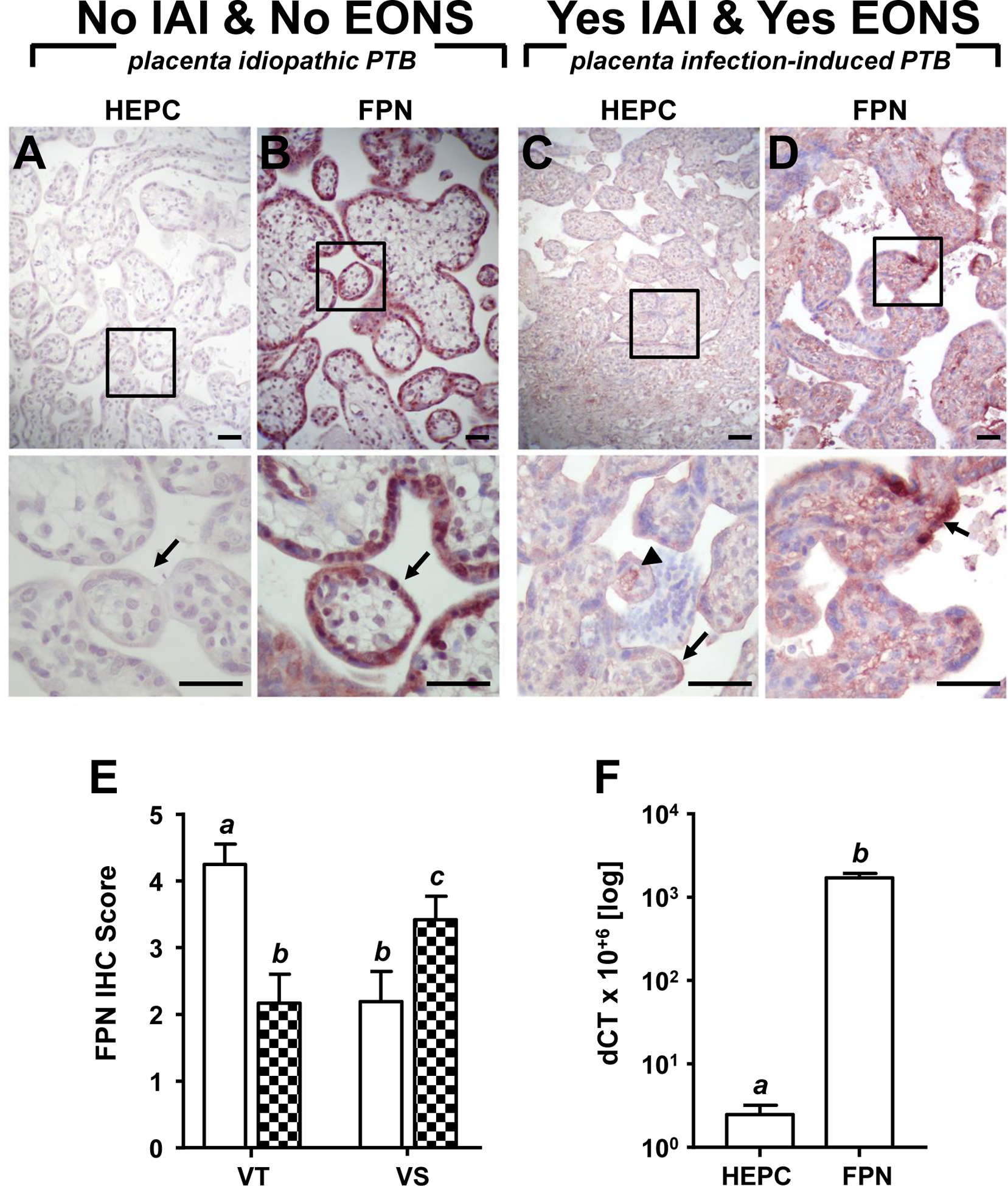
Representative placental immunohistochemical staining of hepcidin (HEPC) and ferroportin (FPN) in idiopathic preterm birth (iPTB, 29 weeks GA at birth) and preterm birth in the context of infection-induced preterm birth (IAI)-determined early-onset sepsis (EONS, 30 weeks GA at birth). (A) Minimal HEPC staining in villous stroma and trophoblast (arrow), and (B) intense FPN restricted to cytotrophoblasts, syncytiotrophoblast and fetal endothelium, delineating villus stroma from maternal and fetal vascular spaces (arrow) observed in iPTB placenta. (C) Intense HEPC staining at apical edge of villi (arrow) and along fetal capillary (arrowhead), and (D) diffuse FPN stained stroma with contiguous patches of intensely stained syncytiotrophoblast (inset, arrow) in IAI placenta. Upper panels, 200× magnification; bottom panels represent boxed region in upper panels, 600× magnification; scale bar = 50 μm (all panels). (E) Semi quantitative score of placental ferroportin staining intensity in villous trophoblast (VT) and villous stroma (VS) in cases of iPTB (open bars, n = 12) and preterm birth in the context of IAI (n = 12, checkered bars). (F) Relative hepcidin and ferroportin mRNA abundance in preterm placenta. Means with different letters are statistically different at a value of p < 0.05.