

Abstract
Background:
Psoriasis is associated with spondyloarthropathy in 10%–30% of cases. Enthesitis is major feature of psoriatic arthritis. Ultrasonography can detect subclinical entheseal abnormalities in psoriasis patients.
Objectives:
To determine the prevalence of subclinical enthesopathy in psoriasis vulgaris using ultrasonography and evaluating its correlation with severity and duration of psoriasis.
Materials and Methods:
This study included 50 patients of psoriasis vulgaris and 50 healthy controls. Sonographic evaluation of six sites bilaterally (proximal plantar fascia, distal Achilles tendon, distal and proximal patellar ligaments, distal quadriceps, and brachial triceps tendons) were done in each subject. All Ultrasonographic findings were identified according to MASEI (Madrid sonography enthesitis index). Enthesopathy scores of patients and controls were compared and receiver operating characteristic curve was used to determine cut off value of MASEI, above which ultrasound enthesitis of clinical significance could be diagnosed.
Results:
31 (62%) psoriasis patients had subclinical enthesopathy of clinical significance as compared to only 5 (10%) of controls. Mean MASEI score between psoriasis cases and control was statistically different, 12.72 ± 7.55 (Mean ± SD) and (5.14 ± 4.69), respectively (P value 0.000001).The receiver operating characteristic curve established an ultrasound score of >11 as the best cut-off to differentiate between subject with enthesopathy of clinical significance from those with enthesopathy of unknown significance. No statistically significant correlation was found between the degree of enthesopathy (MASEI score) and duration and severity of the psoriasis.
Conclusion:
Ultrasonography can effectively screen subclinical entheseal abnormalities in psoriasis patients.
Keywords: Enthesopathy, psoriasis, subclinical, ultrasonography
Introduction
Psoriasis is associated with spondyloarthropathy in 10%–30% of cases.[1] Approximately, 3%–8% patients of psoriasis present with articular symptoms, in the absence of sufficient criteria for the diagnosis of psoriatic arthritis (PsA).[2,3,4] Entheses are the initial site of joint inflammation with most common predilection to lower limbs.[5,6]
High-resolution ultrasound transducers have made it possible to detect entheseal abnormalities, even in clinically silent arthropathy, thus providing a window of opportunity to prevent long-term damage. Earlier studies based on Glasgow ultrasound enthesitis scoring system (GUESS) have described features of lower limb enthesitis.[7] Recently, a new ultrasound enthesis score has been developed—the Madrid sonography enthesitis index (MASEI) containing additional parameters beyond those used by GUESS which includes power Doppler and upper limb examinations.[8] Musculoskeletal ultrasonography is widely available and inexpensive, and readily demonstrates superficial tissue inflammation such as fluid collections, soft tissue lesions, entheseal and tendon abnormalities, as well as bone surface lesions with a sensitivity comparable with magnetic resonance imaging.[9]
The study determines the prevalence of subclinical enthesopathy in patients of psoriasis vulgaris based on MASEI and evaluates its correlation with severity and duration of psoriasis.
Materials and Methods
It was a non interventional case-control study conducted on patients attending the outpatient clinic of a tertiary care center. The study included 50 patients of chronic plaque psoriasis and 50 healthy controls. This study was approved by the Ethics Committee of our institution. Patients were diagnosed to have plaque psoriasis based on clinical and histopathological examination. The psoriasis vulgaris patients, aged more than 18 years were recruited as cases in the study. Patients having history of other rheumatological disorders, trauma, any component of metabolic syndrome or systemic treatment in last 2 months; joint related symptoms or with serological evidence of rheumatoid factor were excluded from the study. Subjects not having psoriasis or any joint-related disorders were recruited as controls. Psoriasis severity was assessed by Psoriasis Area and Severity Index (PASI), Nail psoriasis severity index (NAPSI), and body surface area (BSA) measurements. Clinico-demographic parameters, laboratory investigations, and ultrasound findings of the entheses in cases and controls were recorded as per predesigned proforma. Enthesial ultrasound (US) was performed using standard protocol and with a Logiq P5 and Alpinion ecube 15 EX systems, equipped with a 7–12 MHz broadband linear transducer.[10] US findings were quantified according to the MASEI score, which systematically explores 6 enthesis locations bilaterally (proximal plantar fascia, distal Achilles tendon, distal and proximal patellar ligaments, distal quadriceps, and brachial triceps tendons) in each subject. The sonographic examination evaluated the following characteristics of the enthesis at each site: thickness, structure, calcifications, bursitis, erosions, and power Doppler signal in the bursa or enthesis full tendon (cortical bone profile, intratendon and paratendon on the enthesis insertion) [Figures 1-6]. Total MASEI score was calculated as the sum of scores for both sides (enthesis), with a maximum possible score of 136. MASEI scores were compared between cases and control and were correlated with severity indices of psoriasis.
Figure 1.
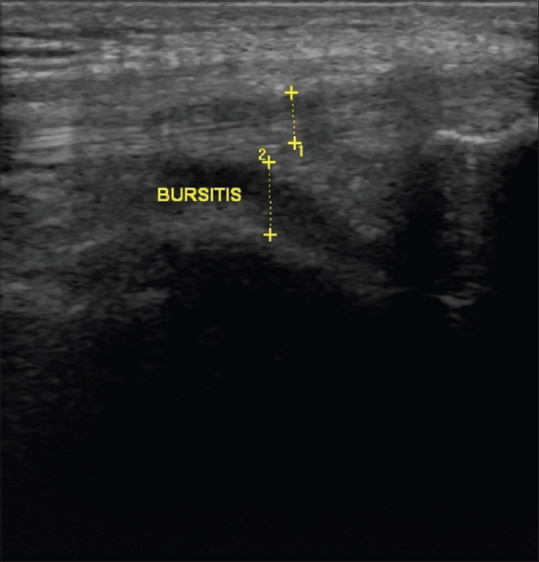
Fluid in retrocalcaneal bursa
Figure 6.
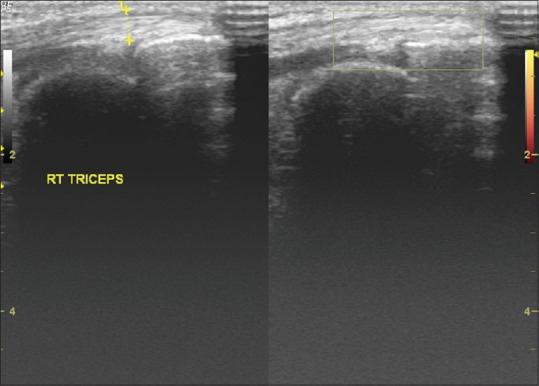
Longitudinal sonography of the triceps tendon shows the normal Doppler signal at the entheseal site
Figure 2.
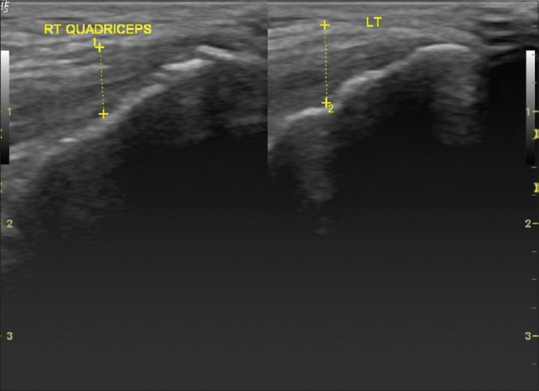
Left quadriceps tendon thickness greater than cut off compared with right quadriceps showing thickness within cut off level
Figure 3.
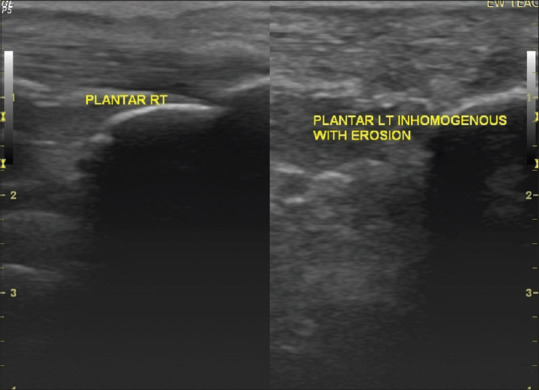
Longitudinal sonography of planter aponeurosis (left) showing loss of fibrillar pattern with underlying erosion as compared with normal (right)
Figure 4.
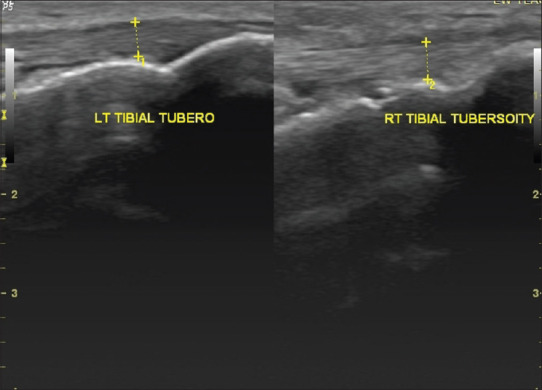
Erosion of the right tibial tuberosity with normal left tibial tuberosity
Figure 5.
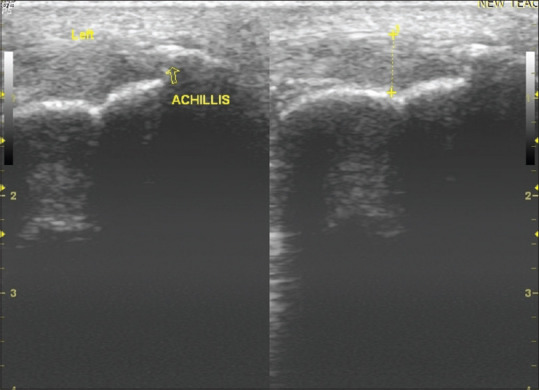
Longitudinal sonography of the left Achilles tendon shows calcifications (arrow) at the entheseal site
Statistical analysis was done with quantitative data expressed as the mean ± SD, and qualitative data expressed as percentages. Mann-Whitney U test was used for comparison of means. Spearman's correlation coefficient (rho) was used for the analysis of correlation. A receiver operating characteristic curve was used to calculate the different levels of sensitivity and specificity at every cutoff point. The statistical significance was set at P < 0.05 throughout.
Results
The groups were comparable in terms of age and gender. The mean age of the case and control groups were 40.50 years and 42.36 years, respectively. Male to female ratio in both case and control groups were similar and were 1.17:1 and 1.08:1, respectively. Duration of psoriasis ranged from3 years to 25 years with mean duration of 8.03 years. Clinico-demographic characteristics for each group of patients and controls are shown in Table 1. Mean MASEI score between psoriasis cases and control was statistically different, (12.72 ± 7.55) (Median 14; IQR 6) and (5.14 ± 4.69) (Median 5; IQR 3.75), respectively (Z score -4.877) (P- value 0.000001) [Table 2]. A total of 1200 enthesis were observed by ultrasound (600 each in cases and control). Enthesopathy was detected most frequently in Achilles tendon of cases with a mean MASEI score of 2.64 ± 1.82 (Median 3: IQR 1). Most common elementary lesion detected was loss of fibrillar pattern, which accounted for 80% in cases and 44% in controls. Least common elementary lesion detected was calcification, seen in 4% of cases but none in controls. There was no power Doppler (PD) flow abnormality in either group.
Table 1.
Clinicodemographic characteristic and elementary lesions of enthesopathy in cases and controls
| Characteristics | Cases (n=50) | Controls (n=50) | P |
|---|---|---|---|
| Age years (mean±SD) | 40.50±13.78 | 42.36±14.25 | 0.50 |
| BMI | 24.20±3.15 | 24.03±2.50 | 0.75 |
| ESR | 13.00±4.50 | 12.76±3.15 | 0.75 |
| FBS (mg/dl) | 85.34±7.99 | 83.26±9.14 | 0.22 |
| Total cholesterol (mg/dl) | 190.86±13.53 | 186.04±12.78 | 0.07 |
| Total triglycerides (mg/dl) | 81.20±23.33 | 83.96±18.54 | 0.51 |
| Serum uric acid (mg/dl) | 4.24±0.98 | 4.23±1.04 | 0.94 |
| Enthesopathy [n%] | 31 (62%) | 5 (10%) | 0.00000006 |
| Elementary lesions of enthesopathy | |||
| Structure inhomogeneity | 40 (80%) | 22 (44%) | 0.0002 |
| Thickness >cut off | 35 (70%) | 15 (30%) | 0.000006 |
| Calcification | 2 (4%) | 0 (0%) | 0.15 |
| Erosion | 4 (8%) | 1 (2%) | 0.17 |
| Bursitis | 10 (20%) | 4 (8%) | 0.08 |
| PD flow abnormality | 0 (0%) | 0 (0%) | 1.00 |
Table 2.
MASEI score (Mean) by enthesis affected
| Enthesis Affected | Cases | Control | P |
|---|---|---|---|
| Plantar fascia | 1.48±1.44 | 0.96±0.94 | 0.113 |
| Achilles tendon | 2.64±1.82 | 1.30±1.23 | 0.0002 |
| Distal patellar tendon | 2.08±2.09 | 1.02±1.22 | 0.016 |
| Proximal patellar tendon | 2.24±1.59 | 0.66±0.91 | 0.00000055 |
| Quadriceps tendon | 2.22±1.64 | 0.80±0.90 | 0.000015 |
| Triceps tendon | 2.06±1.64 | 0.40±0.72 | 0.00000007 |
| Total MASEI scores | 12.72±7.55 | 5.14±4.69 | 0.000001 |
Table 2 shows the MASEI score in each enthesis affected. Psoriasis patients have significantly higher scores than controls when compared at all entheseal sites (all P values <0.05).
Mean disease duration was (8.03 ± 5.81) years (Median 5.25; IQR 4.75). There was no statistically significant correlation between the MASEI score and the duration of psoriasis (r = 0.08; P = 0.58) [Figure 7a].
Figure 7.

Scatter diagrams revealing enthesopathy is independent of (a) Duration; (b) Psoriasis area severity index (PASI); (c) Body surface area involved by psoriasis (BSA); (d) Nail psoriasis severity index (NAPSI)
The severity of psoriasis was measured using PASI, BSA, and NAPSI. Correlation between these severity indices with enthesis score (MASEI) was sought. Mean PASI was 12.42 ± 7.86 (Median 9.45; IQR 8.25). No statistically significant correlation was seen between the MASEI score and the PASI (r = 0.090; P-value = 0.532) [Figure 7b]. Body surface area involved by psoriasis ranged between 4% and 58% (Median 12; IQR 10). There was no statistically significant correlation between the MASEI score and the BSA (r = 0.250; P-value = 0.08) [Figure 7c]. Nail involvement was seen in 26 patients with NAPSI score ranging from 8 to 46 (Median 19.5; IQR 5.75). There was no statistically significant correlation between the MASEI score and the NAPSI (r = 0.090; P value = 0.533) [Figure 7d].
The ROC (Receiver operating characteristic curve) analysis was performed using the overall MASEI score. The MASEI score of >11 was found to differentiate subjects with enthesopathy of clinical significance (Psoriatic arthritis) from that of undetermined significance [Figure 8]. The cutoff point of 11 was exceeded by 31 (62%) subjects in the cases group and 5 (10%) subjects in the control group. Subclinical enthesopathy of significance was found in 62% of psoriasis patient as compared to only 10% of controls.
Figure 8.
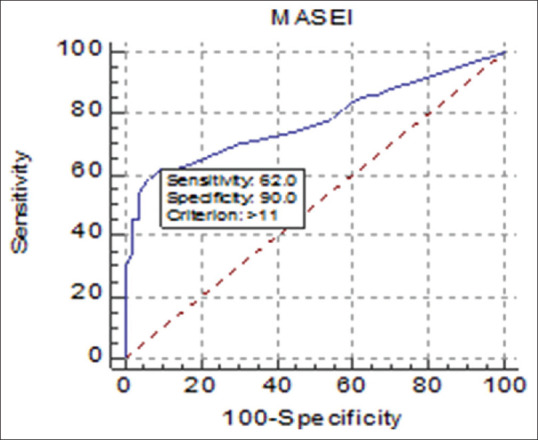
Analysis of cut off of overall MASEI score using ROC curve
Discussion
Psoriatic arthritis (PsA) m is regarded as enthesis associated disorder rather than primary synovitic arthropathy. Ultrasound study may detect the presence of enthesitis in the absence of synovitis in patients of PsA. Our study evaluated the role of entheseal utrasonography in the subclinical diagnosis of psoriatic enthesopathy and arthritis.
Although studies from the past evaluated subclinical enthesopathy in psoriasis using different ultrasonography enthesis scoring like GUESS score, the present study used more precise MASEI scoring for evaluating ultrasound enthesopathy.
This study detected ultrasound entheseal abnormalities of clinical significance in 62% patients with psoriasis as compared to only 10% of controls. The mean MASEI scores of psoriasis group were higher as compared to controls. Similar results were observed in studies by Gisondi et al.[11] and Naredo et al.[12] althoughwith different scoring systems. This could be explained by systemic inflammatory state, associated with psoriasis.
The study emphasizes ultrasonography as a useful tool for detecting subclinical entheseal abnormalities in patients of psoriasis. The results of our study are in agreement with De Filippis et al.[13] This could be explained as ultrasonography is much more sensitive than clinical examination and routine X-ray in depicting subclinical changes in enthesis.
The study observed burden of enthesopathy to be greater in Achilles tendon. Similar observations were noted by Ozcakar et al.[14] The additional mechanical factors may be contributing factor at the site.
Mean MASEI score did not correlate to the duration and severity of psoriasis. These observations are supported by several other studies including Gisondi et al.[11] and Bandinelli et al.[15] No statistically significant differences were found in MASEI score between psoriasis patients with nail involvement as compared to those without nail involvement. This is in contrast to the study by Ash et al.[16] who found significantly higher enthesopathy scores in patients with nail disease than in patients without nail disease, and concluded that nail involvement frequently underlies a systemic subclinical enthesopathy.
Another relevant factor affecting enthesopathy is the BMI. We did not observe any statistically significant difference in both groups in terms of BMI. Mean of serum glucose, cholesterol, triglycerides, and uric acid levels were matched among groups to avoid the effect of confounding factors.[17,18,19,20] Our data confirms that entheseal abnormalities are common in patients with psoriasis without any clinical signs of articular involvement and we suggest that these findings could be related to entheseal inflammation, which is not clinically apparent. To the best of our knowledge, we were unable to find a study in our region to evaluate enthesopathy using MASEI scoring system in psoriasis vulgaris patients. Although MASEI score included elemental lesions of both gray scale and Doppler, it included bursitis as an elemental lesion in the evaluation of enthesitis which is not in agreement with the recently proposed definition of sonological enthesitis by Outcome Measures in Rheumatology (OMERACT). This was a major limitation of our study.
Conclusion
Ultrasonography can be used as a cost-effective screening tool for detecting subclinical enthesopathy. Although a significant correlation between duration and severity of psoriasis vulgaris with enthesopathy could not be derived, studies should be planned to know the significance of ultrasonographic enthesopathy indices in clinical practice.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
Dr. Vishal vyas for contributing for statistical analysis of data.
References
- 1.Girolomoni G, Gisondi P. Psoriasis and systemic inflammation: Underdiagnosed enthesopathy. J Eur Acad Dermatol Venereol. 2009;23:3–8. doi: 10.1111/j.1468-3083.2009.03361.x. [DOI] [PubMed] [Google Scholar]
- 2.Ibrahim G, Waxman R, Helliwell PS. The prevalence of psoriatic arthritis in people with psoriasis. Arthritis Rheum. 2009;61:1373–8. doi: 10.1002/art.24608. [DOI] [PubMed] [Google Scholar]
- 3.Zanolli MD, Wikle JS. Joint complaints in psoriasis patients. Int J Dermatol. 1992;31:488–91. doi: 10.1111/j.1365-4362.1992.tb02696.x. [DOI] [PubMed] [Google Scholar]
- 4.Stern RS. The epidemiology of joint complaints in patients with psoriasis. J Rheumatol. 1985;12:315–20. [PubMed] [Google Scholar]
- 5.McGonagle D, Gibbon W, Emery P. Classification of inflammatory arthritis by enthesitis. Lancet. 1998;352:1137–40. doi: 10.1016/S0140-6736(97)12004-9. [DOI] [PubMed] [Google Scholar]
- 6.McGonagle D, Gibbon W, O’Connor P, Green M, Pease C, Emery P. Characteristic magnetic resonance imaging entheseal changes of knee synovitis in spondylarthropathy. Arthritis Rheum. 1998;41:694–700. doi: 10.1002/1529-0131(199804)41:4<694::AID-ART17>3.0.CO;2-#. [DOI] [PubMed] [Google Scholar]
- 7.Gutierrez M, Filippucci E, De Angelis R, Salaffi F, Filosa G, Ruta S, et al. Subclinical entheseal involvement in patients with psoriasis: An ultrasound study. Semin ArthritisRheum. 2011;40:407–12. doi: 10.1016/j.semarthrit.2010.05.009. [DOI] [PubMed] [Google Scholar]
- 8.De Miguel E, Cobo T, Munoz-Fernandez S, Naredo E, Uson J, Acebes JC, et al. Validity of enthesis ultrasound assessment in spondyloarthropathy. Ann Rheum Dis. 2009;68:169–74. doi: 10.1136/ard.2007.084251. [DOI] [PubMed] [Google Scholar]
- 9.Kamel M, Eid H, Mansour R. Ultrasound detection of knee patellar enthesitis: A comparison with magnetic resonance imaging. Ann Rheum Dis. 2004;63:213–4. doi: 10.1136/ard.2003.010314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Frediani B, Falsetti P, Storri L, Allegri A, Bisogno S, Baldi F, et al. Quadricepital tendon enthesitis in psoriatic arthritis and rheumatoid arthritis: Ultrasound examinations and clinical correlations. J Rheumatol. 2001;28:2566–8. [PubMed] [Google Scholar]
- 11.Gisondi P, Tinazzi I, El-Dalati G, Gallo M, Biasi D, Barbara LM, et al. Lower limb enthesopathy in patients with psoriasis without clinical signs of arthropathy: A hospital-based case-control study. Ann Rheum Dis. 2008;67:26–30. doi: 10.1136/ard.2007.075101. [DOI] [PubMed] [Google Scholar]
- 12.Naredo E, Moller I, De Miguel E, Batlle-Gualda E, Acebes C, Brito E, et al. High prevalence of ultrasonographic synovitis and enthesopathy in patients with psoriasis without psoriatic arthritis: Aprospective case-control study. Rheumatology. 2011;50:1838–48. doi: 10.1093/rheumatology/ker078. [DOI] [PubMed] [Google Scholar]
- 13.De Filippis LG, Caliri A, Lo Gullo R, Bartolone S, Miceli G, Cannavo SP, et al. Ultrasonography in the early diagnosis of psoriasis-associated enthesopathy. Int J Tissue React. 2005;27:159–62. [PubMed] [Google Scholar]
- 14.Ozcakar L, Cetin A, Inanici F, Kaymak B, Gurer CK, Kolemen F. Ultrasonographical evaluation of the Achilles’ tendon in psoriasis patients. Int J Dermatol. 2005;44:930–2. doi: 10.1111/j.1365-4632.2004.02235.x. [DOI] [PubMed] [Google Scholar]
- 15.Bandinelli F, Prignano F, Bonciani D, Bartoli F, Collaku L, Candelieri A, et al. Ultrasound detects occult entheseal involvement in early psoriatic arthritis independently of clinical features and psoriasis severity. Clin Exp Rheumatol. 2013;31:219–24. [PubMed] [Google Scholar]
- 16.Ash ZR, Tinazzi I, Gallego Cc, KwokC, Wilson C, Goodfield M, et al. Psoriasis patients with nail disease have a greater magnitude of underlying systemic subclinical enthesopathy related arthritisthan those with normal nails. Ann Rheum Dis. 2012;71:553–6. doi: 10.1136/annrheumdis-2011-200478. [DOI] [PubMed] [Google Scholar]
- 17.Descamps OS, Leysen X, Van Leuven F, Heller FR. The use of Achilles tendon ultrasonography for the diagnosis of familial hypercholesterolemia. Atherosclerosis. 2001;157:514–8. doi: 10.1016/s0021-9150(01)00533-0. [DOI] [PubMed] [Google Scholar]
- 18.Akturk M, Ozdemir A, Maral I, Yetkin I, Arslan M. Evaluation of achilles tendon thickening in type 2 diabetes mellitus. Exp Clin Endocrinol Diabetes. 2007;115:92–6. doi: 10.1055/s-2007-955097. [DOI] [PubMed] [Google Scholar]
- 19.Schweitzer ME, Karasick D. MR imaging of disorders of the Achilles tendon. Am J Roentgenol. 2000;175:613–25. doi: 10.2214/ajr.175.3.1750613. [DOI] [PubMed] [Google Scholar]
- 20.Civeira F, Castillo JJ, Calvo C, Ferrando J, de Pedro C, Martinez-Rodes P, et al. Achilles tendon size by high resolution sonography in healthy population. Relationship with lipid levels. Med Clin (Barc) 1998;111:41–4. [PubMed] [Google Scholar]