
Figure 5. Immunofluorescence staining confirms that pressure overload greatly promotes RVCM proliferation.
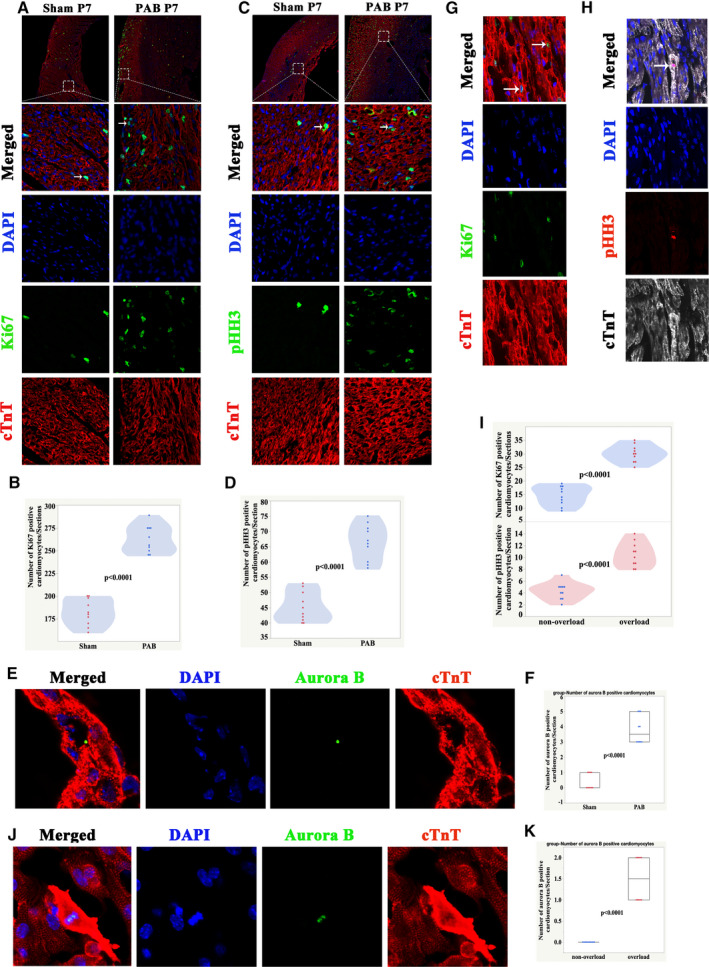
A, Immunofluorescence staining for Ki67 (green), cardiac troponin T (red), and DAPI (blue) in rats at P7. B, Quantification of Ki67‐positive cardiomyocytes at P7, n=10 samples. C, Immunofluorescence staining for pHH3 (green), cTnT (red), and DAPI (blue) in rats at P7. Arrows indicate proliferating cardiomyocytes. D, Quantification of pHH3‐positive cardiomyocytes, n=10 samples. E, Immunofluorescence staining for aurora B (green), cTnT (red), and DAPI (blue) in rats at P7. F, Quantification of aurora B‐positive cardiomyocytes at P7. G, Representative Ki67‐positive cardiomyocytes from patients with RV pressure overload. Ki67 (green), cardiac troponin T (red), and DAPI (blue). Arrows indicate proliferating cardiomyocytes. H, Representative pHH3‐positive cardiomyocytes from patients with RV pressure overload. pH3 (red), cTnT (white), and DAPI (blue). Arrows indicate proliferating CMs. I, Quantification of Ki67/pHH3‐positive cardiomyocytes in human samples. J, Representative Ki67‐positive cardiomyocytes from patients with RV pressure overload. Aurora B (green), cTnT (red), and DAPI (blue). K, Quantification of aurora B‐positive cardiomyocytes in human samples. CMs indicates cardiomyocytes; cTnT, cardiac troponin T DAPI, 4′,6‐diamidino‐2‐phenylindole; PAB, pulmonary artery banding; pHH3, phospho‐histone H3; RV, right ventricle; and RVCM, right ventricular cardiomyocyte.