

Abstract
While virus epidemics are nothing new to man, the scale, speed of global spread and immediacy of the COVID-19 pandemic have been truly unprecedented [1]. The entire world has been turned on its head in less than a few months, with major implications beyond disease burden and loss of life, threatening the economic status quo and human psychosocial balance and wellbeing not only for patients, but for all of us. The primary aim of our Call for Action Viewpoint was to support and protect our adult congenital heart disease (ACHD) patients and their needs during these challenging and uncertain times. This goal had to be met while we, as individuals, teams, institutions and nations, came together in a global effort to combat this aggressive virus, that appears to spare no organs or systems, nor any borders, geographic or other. As with any crisis, there is always opportunity: we are submitting herewith a vision for a different and better model of ACHD care, and for a better life journey and health care experience for our patients, that should be in place in the aftermath of the Covid-19 pandemic. Many of the points and principles discussed in this article, need not be confined to ACHD patients, but have a broader reach. And we must not forget nor neglect the most vulnerable in society at this time, namely the elderly, disabled and other dependent or disadvantaged groups in this “We Are One” global operation. Last but not least, this maybe the time to take better care of ourselves (and others) and reflect on life.
Keywords: Covid-19, Pandemic, Adult congenintal heart disease, New health care model, Patient education, Patient empowerment
We are currently through a phase of slow and painful understanding of the epidemiology, clinical spectrum and risk profile of Covid-19 [1], this knowledge shared by emerging, fast-track scientific publications [[2], [3], [4]]. To our knowledge, there is only anecdote concerning ACHD specific data at present. However, there is institutional and regional experience, for example from Lombardy [5], and a global collaborative effort to ascertain the disease profile and its impact on ACHD [6], albeit the latter will take time to fruition. The heterogeneity of our population represents an additional challenge; defining risk and making recommendations about social behaviour in ACHD has to be individualized. Studies are currently underway regarding COVID-19 specific data on ACHD and other cardiovascular disease, looking at epidemiology, risk and interaction with medications, such as ACEi. Furthermore, there are numerous drug trials and a global effort to develop better testing and new vaccines specific to Covid-19 that should benefit us all in the coming 6 months to a year. There is, nevertheless, an imperative right now to provide direction for the ACHD community (and to other patient groups) on best practice and at the same time, we submit herewith, to portray a future model of care more aligned to the 21st century, utilizing technology to provide a smoother and richer life experience for ACHD patients.
1. Number one priority: protect and support ACHD care and continue to provide for ongoing, short and longer-term patients' needs
-
•
Social distancing [7] (a misnomer; should read physical distancing …) seems now to be more or less universaly accepted and enforced in the so called developed world to slow down the spread of Covid-19 3, so that health care systems increase capacity and become able to accommodate and support the minority of patients -at the critical end of the Covid spectrum-requiring intensive care therapy. This delay in the spread of the disease may also enable a slower form of ‘herd immunity’ to occur (with less human loss) and allow time for Covid specific therapies and vaccines to develop, thus ultimately leading to the containment of the pandemic. All ACHD patients as the rest of us, should follow this rule, until further notice.
-
•
Are ACHD patients high-risk should they contract Covid-19? Pre-existing cardiovascular disease increases vulnerability to COVID-19 albeit, this has not yet been shown in the context of ACHD. Older age has also been a risk factor for Covid-19 outcomes; in this regard, ACHD patients are a younger adult group and thus, may have a relative advantage. It has been suggested, nevertheless, that patients with complex underlying congenital heart disease (such as single ventricle [with a Fontan palliation or not], patients with chronic cyanosis, a systemic right ventricle, pulmonary arterial hypertension (PAH), decompensated heart failure, previous heart and or lung transplantation and immunocompromised patients (small minority in ACHD, such as patients with Di George or Down syndrome) are particularly vulnerable 8. These patients should be ‘shielded’ for a period of 12 weeks or until further notice. Co-morbidity, cardiac or not, has been shown to be a risk factor for Covid outcomes in non-ACHD cohorts, and this may well be applicable to ACHD patients too. Some of these factors such as smoking, obesity, systemic hypertension, diabetes are modifiable and can be actively addressed during this period of self isolation (between the 1st and the second ‘wave’ of the pandemic, whenever the latter comes, if it does so).
-
•
Rapid conversion of outpatient clinics to digital clinics and deferment of non-urgent/planned operations (surgical, catheter or other) to protect ACHD patients from Covid-19 exposure. Tele- or Video-clinics are now standard, functional and have been well received by ACHD patients globally. Moreover, they may substitute rather than replace conventional face-to-face clinics [9,10] in a revised, hybrid model of care beyond the Covid-19 pandemic. Defering elective operations [11], should not necessarily compromise long-term prospects for ACHD patients in the short-term, provided that provisions are made to accommodate the anticipated increased need in the medium to long-term, as the pandemic eases. Creating „green zones“ for allowing non-urgent ACHD work to restart has been in some ways more problematic than the rapid coversions to combat the Covid threat. This is largely due to health care planners being adamant in ring fencing capacity for potential subsequent Covid waves, not yet materilaized.
-
•
Provisions made and communicated widely regarding urgent ACHD inpatient care (medical, catheter based and or surgical). It was obviously paramount, that in the frenzied effort to combat the Covid-19 pandemic, urgent needs of ACHD patients [12,13] (and other tertiary patient cohorts' needs) were not overlooked nor neglected. While, many ACHD patients that would normally attend tertiary centres for non-scheduled rapid assesment and care [14] may be potentially managed at home or with local and community medical and nursing input -under close guidance and remote supervision from ACHD teams-there are still some, highly selected ACHD patients, that must be admitted and receive tertiary inpatient care. Such space and capacity must be well defined and ring fenced for each tertiary ACHD centre and be provided for non-Covid and/or Covid ACHD urgent needs, on an individualized patient base. For example, Harefield Hospital [15] is designated as the ACHD Cardiac Surgical Hub within the primary author's London NHS Trust for the period of the pandemic, while the Royal Brompton Hospital has been largely converted into a Covid centre. At the same time, all Paediatric Invasive Cardiac work has been temporarily relocated to Evelina London Children's Hospital, to increase Covid capacity at the Brompton end. Collaboration across all ACHD professional groups and centres will be important in ensuring access to the right care for individual patients. On this point, it must be emphasized that full congenital heart disease capacity and service are expected by our patients and their families and must be resumed at the end of the pandemic; health care planners, providers and we, as the profession, will be judged should we fail to realize this.
-
•
Timely and multi-facet communication with ACHD patients with regular updates are key. At such unsettling times, sharing information about Covid-19 with patients and their families, as it emerges, providing guidance and reassurance and making them aware of infrastructures in place for their urgent and long-standing needs and of our planning for longer term ACHD service provision and improvements post-Covid are all necessary. We have utilized our institutional and other legitimate professional and national health care websites [7] to achieve this, together with free access scientific papers [1,8], employment of social media, the establishment of the ACHD Forum 2020 and, in close collaboration with the patient association/s and the patients themselves, the running of Live Webinars widely attended by global audiences and accessible on the Internet (see footnote of this article). As lockdown measures start relaxing in some countries, the so called “extreme vulnerable group” including a minority of ACHD patients must have one-to-one discussions with their ACHD physician on returning to work and the new normal. An individualized approach is clearly necessary here respecting relative risks, nature of work, access to it and crucially, the patient's social circumstances and views.
1.1. Clinical vignettes and triaging of ACHD patients to tertiary vs community care in the Covid era
A). Our first Covid +ve patient was a 61-year-old gentleman admitted from the community with rising CRP levels and the assumption of resurgence of fungal sepsis, following major cardiac surgery for fungal endocarditis and a protracted hospital stay but eventual discharge on oral antifungal therapy, 3 weeks prior to readmission. A surprising Covid +ve admission swab, and a history of temporary loss of taste at home, but no other overt systemic disturbance followed by normalization of CRP in a matter of days, showing in this single case that Covid-19 infection may have a subclinical course in a Caucasian patient of mature age (for ACHD), despite pre-existing left ventricular dysfunction and concomitant renal disease. B). New onset atrial flutter in a 45-year-old female patient with congenitally corrected transposition of the great arteries and a mechanical tricuspid valve prosthesis, that we would normally admit for DC cardioversion, who was managed remotely with amiodarone loading followed by a small dose of b-blockers and doing well and feeling better at present and, under review. The learning point in her case is that atrial flutter was misdiagnosed [16] as sinus tachycardia at the local accident and emergency department until she made contact with us, when atrial flutter was revealed, emphasizing the need for vigilant ACHD input if we are to manage our patients remotely. C). Such need for close input and supervision is also highlighted in two ACHD patients with decompensated heart failure [14] at the two ends of the age spectrum: a) a 18-year-old male with a failing Fontan, chronic ascites who had temporary symptomatic relief with periodic abdominal paracenteses, now being managed effectively with fluid restriction and the addition of metolazone and b) a 77-year-old gentleman with history of multiple aortic valve surgeries, impaired left ventricular function and amyloidosis, now managed at home with our 24/7 input in conjunction with the community and palliative care teams. We submit such strategies of managing ACHD patients outside of the tertiary setting, may be effective albeit they require close supervision and support from the tertiary centre and will rely heavily on community/local hospital resources. Equally, clear communication amongst all parties involved is key. Nevertheless, some patients will require tertiary inpatient care, no matter what, and provision for them must be in place.
2. Other needs in the Covid era
-
•
Mental and psychosocial wellbeing of the ACHD patient and of the workforce: [17] First of all, we must acknowledge that we are not alone in this pandemic [5]. Second, social distancing should be seen as an opportunity for social embracing i.e. coming closer as human beings, in addition to physical distancing, utilizing the wonders of the digital world and technology to effect it. This is our chance to spend time with family, friends and colleagues and be more considerate of others, more tolerant of them and of our selves. To that effect, we have now established The Brompton Fellows Club, an inclusive forum for current and former Fellows and Trainees to foster social interaction, with the condition that Covid can only occupy a small part of the Club sessions. We should also accept, that in these stressful and uncertain times our whole lives have been turned on its head, some of us will need help, and help is available, should we should ask for it and we must.
-
•
Coping mechanisms: ACHD patients (and their families) have solid coping mechanisms already in place, having endured the diagnosis of congenital heart disease in the first instance, undergone multiple operations, uncertainty about their long-term outlook and, for some, physical disability. Yet remarkably, most of them have such a positive outlook to life, a true inspiration for us all.
-
•
Improving oneself: It is as good a time to spend time with ourselves, decide what we would like to make out of this period of turmoil. Take up a hobby, arts and crafts maybe, give up smoking, improve our diet, optimize our weight and crucially, maintain if not improve our physical fitness. We must improvise for the latter, particularly if we live in urban spaces, although some of the lockdown measures are now slowly relaxed in Europe. There are multiple digital or media aids to exercise to choose from. Minimizing daily news consumption is also important, pick up and read a book instead.
3. Beyond the Covid era: opportunities and planning ahead
-
•
A New Model of ACHD Care (Fig. 1 ): Essential elements of this model of care should be: Personalized ACHD Care with Patient Education and Empowerment [18], Life-Style Modification and Equity of Care at heart and the Broader Utilization of Technology to support health care delivery, decision making and research [[19], [20], [21]]. We have argued for such an advanced model for some time. [22] The Covid pandemic has led, of necessity, to the destruction of the previous, outdated model, consisting of bringing patients to outpatient clinics at pre-set intervals, submitting them to prognostic investigations, trying to co-ordinate the results of these, then reaching consensus on best action plans, communicating these plans with the patient before eventually effecting them, clearly a slow and frustrating route for the patients and for us, the providers. We are right now faced with a unique opportunity to build something much better and more 21stCentury. We and others have shown how artificial intelligence, for example, can help us risk stratify ACHD patients [19]and analyse imaging [20,21], providing us with volumetric data on the spot, key elements to decision making in ACHD, we must now apply them in our practice. Our personalized ACHD care model includes a single day visit at the ACHD hub for all patients, including those transitioned from paediatric care, where a comprehensive and thorough assessment of the patient takes place including imaging, cardiopulmonary exercise testing (or 6MWDT), biomarkers/biobanking; the patient is risk starified, sees the Consultant and the Clinical Nurse Specialist and empowered with all necessary information about her/his condition, prognosis, life-style and family planning/contraception etc. Subsequent follow-up is individualized; patients at the good end of the spectrum may be monitored remotely and attend the ACHD hub very infrequently. Patients at the severe end of the spectrum will require closer surveillance, but again some of it can be remote, the heart failure paradigm may be employed here, albeit there is a need to validate it first in ACHD. Most patients should be offered a choice between face-to-face, vs digital clinics vs remote monitoring or a combination of any of these follow-up models. Fast access to ACHD databases with automatic notifications regarding specific action/s that need to be taken by individual patients need to be developed. Patient education and empowerment are essential to optimal ACHD life-long care [18], we must do better on this front. There is no reason that our young patient from the clinical vignettes should not have had copies of her resting ECG in her mobile and a plan of action for atrial tachycardia in her ACHD app - to be developed-to assist the young colleague in the accident and emergency department who mistakenly sends the patient home with a false diagnosis of sinus tachycardia. Physicians will always need to be mindful, using their diagnostic skills, not to overlook other causes for illness; for our patients not every fever or cough means COVID-19. The merits of Lifestyle Modification, including the new mantra of “slim and athletic”, with its consequent effects on the immune system, autonomic nervous function/arrhythmia propensity and overall well-being, highly relevant right now with the pandemic and its associated restrictions, and beyond. This mantra of optimal weight and daily exercise may in fact be the best preparation against a potential Covid infection, we speculate, until a vaccine becomes available. The merits of healthy diet and exercise, in turn must be introduced to families and patients early in life though. Last but not least, we are aware and working towards resolving ACHD care inequalities within Networks; again technology, remote monitoring and patient education and empowerment are all necessary to succeed in this noble cause, so that every patient diagnosed with CHD, anywhere within a given Network has access to equitable ACHD care and best prospects to life.
Fig. 1.
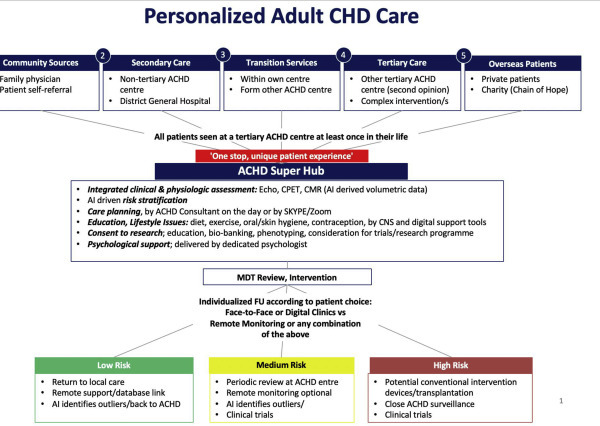
Personalized ACHD care model. Modified from Brida M, Gatzoulis MA Acta Paediatrica 2019;108(10):1757–64 (with permission). ACHD, adults with congenital heart disease; AI, artificial intelligence; CHD, congenital heart disease; CMR, cardiac magnetic resonance; CNS, clinical nurse specialist; CPET, cardiopulmonary exercise testing; Echo, echocardiography; FU, follow-up; MDT, multidisciplinary team.
In summary, we all had to make major life adaptations in response to the Covid-19 pandemic, including rapid changes to ACHD practice. While there is optimism that, with time, we will succeed in our efforts to contain this global threat, we as professionals must not lose sight of our primary responsibility, that is the care and wellbeing of the ACHD patient. At the other end of this storm, we should have a different, more humane and considerate world that amongst other things provides a much better model of personalized and equitable ACHD care, utilizing technology and educating and empowering patients so that they can reach and enjoy full and independent lives.
Conflict of interest
No conflicts of interest.
Key Points.
The Covid-19 pandemic despite its major, adverse impact on global public health, loss of life and threat to our social-economic fabric will not be here for ever.
Patients with CHD should follow rules on social distancing and those with severe disease (see text) shield themselves to protect from Covid-19 exposure. As Covid-19 restrictions start relaxing in some countries, patients with severe CHD, also called “extreme vulnerable group”, must have one-to-one discussions with their ACHD physician on returning to work and to the new normal.
The best way to arm one-self against a poor outcome in case of contacting Covid-19 in future is to optimize weight, improve diet, increase exercise/physical fitness and maintain mental health (until a vaccine is developed). These measures should also improve long term outlook and quality of life for patients and all, irrespective of the pandemic. Patients with CHD and their families have strong resilience mechanisms in place.
Draconian health care measures/changes to address the Covid-19 pandemic have led to destruction of health care models for chronic disease, including ACHD. This is a unique opportunity to create a new, 21st century Personalized ACHD Care Model, utilizing Technology and Patient Education and Empowerment, promoting Life-Style Changes and Equity of Care, that we are currently working on.
Footnotes
PS. We thank Rob Nicoll, Trustee of The Somerville Foundation and Rachel Adam-Smith, ACHD patient who participated at the ACHD Forum 2020 Webinar on the April 8, 2020 facilitated by LiveMedia https://youtu.be/4swxEJefDBQ for their critique on our manuscript.
References
- 1.Brida M., Chessa M., Gu H., Gatzoulis M.A. The globe on the spotlight: coronavirus disease 2019 (Covid-19) Int J Cardiol. 2020 Apr 3;S0167-5273(20) doi: 10.1016/j.ijcard.2020.04.006. 31727-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Huang C., Wang Y., Li X., et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Li Q., Guan X., Wu P., et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med. 2020:1–9. doi: 10.1056/NEJMoa2001316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wu C., Chen X., Cai Y., et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2020:1–10. doi: 10.1001/jamainternmed.2020.0994. http://www.ncbi.nlm.nih.gov/pubmed/32167524 Available from: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Senni M. COVID-19 experience in Bergamo, Italy. Eur Heart J. 2020 Apr 7 doi: 10.1093/eurheartj/ehaa279. [Online ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Linschoten M., Asselbergs F.W. On behalf of CAPACITY-COVID collaborative consortium. Eur Heart J. 2020 doi: 10.1093/eurheartj/ehaa280. [Online ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.UK government official guidance on Coronavirus outbreak. UK government official website, https://www.gov.uk/coronavirus.
- 8.Tan W.M., Aboulhosn J. The cardiovascular burden of coronavirus disease 2019 (COVID-19) with a focus on Congenital Heart Disease. Int J Cardiol. 2020 Jun 15;309:70–77. doi: 10.1016/j.ijcard.2020.03.063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Baumgartner H., Budts W., Chessa M., Deanfield J., Eicken A., Holm J., Iserin L., Meijboom F., Stein J., Szatmari A., Trindade P.T., Walker F. Working group on grown-up congenital heart disease of the European society of cardiology. Recommendations for organization of care for adults with congenital heart disease and for training in the subspecialty of 'grown-up congenital heart disease' in Europe: a position paper of the working group on grown-up congenital heart disease of the European society of cardiology. Eur Heart J. 2014 Mar;35(11):686–690. doi: 10.1093/eurheartj/eht572. [DOI] [PubMed] [Google Scholar]
- 10.Kempny A., Diller G.P., Dimopoulos K., Alonso-Gonzalez R., Uebing A., Li W., Babu-Narayan S., Swan L., Wort S.J., Gatzoulis M.A. Determinants of outpatient clinic attendance amongst adults with congenital heart disease and outcome. Int J Cardiol. 2016 Jan 15;203:245–250. doi: 10.1016/j.ijcard.2015.10.081. [DOI] [PubMed] [Google Scholar]
- 11.Baumgartner H., Bonhoeffer P., De Groot N.M., de Haan F., Deanfield J.E., Galie N., Gatzoulis M.A., Gohlke-Baerwolf C., Kaemmerer H., Kilner P., Meijboom F., Mulder B.J., Oechslin E., Oliver J.M., Serraf A., Szatmari A., Thaulow E., Vouhe P.R., Walma E. Task force on the management of grown-up congenital heart disease of the European society of cardiology (ESC); association for European paediatric cardiology (AEPC); ESC committee for practice guidelines (CPG). ESC guidelines for the management of grown-up congenital heart disease (new version 2010) Eur Heart J. 2010 Dec;31(23):2915–2957. doi: 10.1093/eurheartj/ehq249. [DOI] [PubMed] [Google Scholar]
- 12.Stout K.K., Daniels C.J., Aboulhosn J.A., Bozkurt B., Broberg C.S., Colman J.M., Crumb S.R., Dearani J.A., Fuller S., Gurvitz M., Khairy P., Landzberg M.J., Saidi A., Valente A.M., Van Hare G.F. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol. 2019 Apr 2;73(12):e81–e192. doi: 10.1016/j.jacc.2018.08.1029. [DOI] [PubMed] [Google Scholar]
- 13.Chessa M., Baumgartner H., Michel-Behnke I., Berger F., Budts W., Eicken A., Søndergaard L., Stein J., Wiztsemburg M., Thomson J. ESC working group position paper: transcatheter adult congenital heart disease interventions: organization of care – recommendations from a joint working group of the European society of cardiology (ESC), European association of pediatric and congenital cardiology (AEPC), and the European association of percutaneous cardiac intervention (EAPCI) Eur Heart J. 2019 Apr 1;40(13):1043–1048. doi: 10.1093/eurheartj/ehy676. [DOI] [PubMed] [Google Scholar]
- 14.Budts W., Roos-Hesselink J., Rädle-Hurst T., Eicken A., McDonagh T.A., Lambrinou E., Crespo-Leiro M.G., Walker F., Frogoudaki A.A. Treatment of heart failure in adult congenital heart disease: a position paper of the working group of grown-up congenital heart disease and the heart failure association of the European society of cardiology. Eur Heart J. 2016 May 7;37(18):1419–1427. doi: 10.1093/eurheartj/ehv741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gatzoulis M.A. Adult congenital heart disease at the Royal Brompton: a historical perspective and future directions. Eur Heart J. 2018 Dec 1;39(45):3990–3992. doi: 10.1093/eurheartj/ehy703. [DOI] [PubMed] [Google Scholar]
- 16.Cordina R., Nasir Ahmad S., Kotchetkova I., Eveborn G., Pressley L., Ayer J., Chard R., Tanous D., Robinson P., Kilian J., Deanfield J.E., Celermajer D.S. Management errors in adults with congenital heart disease: prevalence, sources, and consequences. Eur Heart J. 2018 Mar 21;39(12):982–989. doi: 10.1093/eurheartj/ehx685. [DOI] [PubMed] [Google Scholar]
- 17.Kovacs A.H., Bandyopadhyay M., Grace S.L., Kentner A.C., Nolan R.P., Silversides C.K., Irvine M.J. Adult Congenital Heart Disease-Coping and REsilience (ACHD-CARE): rationale and methodology of a pilot randomized controlled trial. Contemp Clin Trials. 2015 Nov;45(Pt B):385–393. doi: 10.1016/j.cct.2015.11.002. [DOI] [PubMed] [Google Scholar]
- 18.Gatzoulis M.A. Adult congenital heart disease: education, education, education. Nat Clin Pract Cardiovasc Med. 2006;3(1):2–3. doi: 10.1038/ncpcardio0382. [DOI] [PubMed] [Google Scholar]
- 19.Diller G.P., Kempny A., Babu-Narayan S.V., Henrichs M., Brida M., Uebing A., Lammers A.E., Baumgartner H., Li W., Wort S.J., Dimopoulos K., Gatzoulis M.A. Machine learning algorithms estimating prognosis and guiding therapy in adult congenital heart disease: data from a single tertiary centre including 10 019 patients. Eur Heart J. 2019 Apr 1;40(13):1069–1077. doi: 10.1093/eurheartj/ehy915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Diller G.P., Babu-Narayan S., Li W., Radojevic J., Kempny A., Uebing A., Dimopoulos K., Baumgartner H., Gatzoulis M.A., Orwat S. Utility of machine learning algorithms in assessing patients with a systemic right ventricle. Eur Heart J Cardiovasc Imag. 2019 Aug 1;20(8):925–931. doi: 10.1093/ehjci/jey211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Diller G.P., Lammers A.E., Babu-Narayan S., Li W., Radke R.M., Baumgartner H., Gatzoulis M.A., Orwat S. Denoising and artefact removal for transthoracic echocardiographic imaging in congenital heart disease: utility of diagnosis specific deep learning algorithms. Int J Cardiovasc Imag. 2019 Dec;35(12):2189–2196. doi: 10.1007/s10554-019-01671-0. [DOI] [PubMed] [Google Scholar]
- 22.Brida M., Gatzoulis M.A. Adult congenital heart disease: past, present and future. Acta Paediatr. 2019;108(10):1757–1764. doi: 10.1111/apa.14921. [DOI] [PubMed] [Google Scholar]