
| APPENDIX | ||
| DESCRIPTION OF MANUAL THERAPY INTERVENTIONS | ||

|

|
|
| (1) Neck accessory mobilization technique | (2) Mobilization neck central | (3) Mobilization up neck |
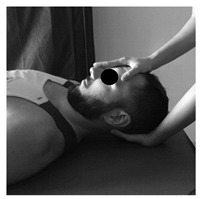
| Patient lies sitting. Non-thrust facet joint distraction mobilization is applied. Clinician left hand separates right lower facet of C7 away from top facet of T1; right hand maintains ventral and medial pressure against lower facet of C7 and compresses it against T1 thus facilitating greater motion on right side of the C7. Manual stabilization of T1 occurs by using the right lower extremity passively, which rotates the T1 segment in opposite direction of the intended mobilization. | Patient lies prone. The posterior-anterior mobilization of the C5 vertebra is carried out. The tips of the clinician’s thumbs are positioned on the spinous process of C5 and an oscillatory pressure is applied in the postero-anterior direction. This mobilization is carried out with a frequency of 2 oscillations per second (2 Hz), with a total of 9 min. The time was distributed in 3 series of 3 min, with 1 min of rest between them. | Patient lies supine. The mobilization is done with one hand in the occipital to perform head traction, and another in the frontal region to apply caudal pressure. This mobilization is carried out at a slow pace of 2 s per oscillation, with a total time of 10 min. |

|

|

|
| (4) Suboccipital inhibition technique | (5) Suboccipital accessory mobilization technique | (6) Trigger points technique |
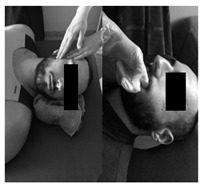
| Patient lies supine. Contact is made with the hands in the occiput. A progressive and deep pressure is applied with the fingertips on the rear arc of the atlas in the direction of the ceiling with slight traction in a cranial direction for 2 min. | Patient lies supine, head turned to the side with slight lateroflexion and neutral flexion-extension. A gentle cephalic decompression is applied, then small circumductions until joint barrier is reached and then a rotation is performed with cranial helical movement. 2 times on each side without passing the joint barrier. | Patient lies supine. Inhibitory pressure is performed on the most sensitive trigger point of the muscles: masseter, temporal and sternocleidomastoid. Gradual pressure is exerted until the onset of pain and maintained 90 s. |
|

|

|
| (7) Myofascial technique | (8) Temporomandibular Joint Mobilization technique | (9) Temporomandibular massage |
| Patient lies supine. (a) One hand is placed in the zygomatic arch and the other one makes slow longitudinal movements on the masseter muscle for 5 min. (b) The index finger is introduced in the last molar and pressure is applied in the posterior and cephalic direction in the region of the lateral and medial pterygoid for 5 s in each. | Patient lies supine. 5 mobilizations are made, introducing the thumb in the area of the lower molars applying a caudal traction force taking the mandibular branch with the rest of the fingers. With the opposite hand, the clinician stabilizes the patient’s forehead. | Patient lies supine. Superficial and deep synchronized frictions, compressions and kneading are performed with moderate pressure on the anterior temporal, masseter and sternocleidomastoid muscles, bilaterally for 2 min. |
Official websites use .gov
A
.gov website belongs to an official
government organization in the United States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you've safely
connected to the .gov website. Share sensitive
information only on official, secure websites.