
Fig. 12.
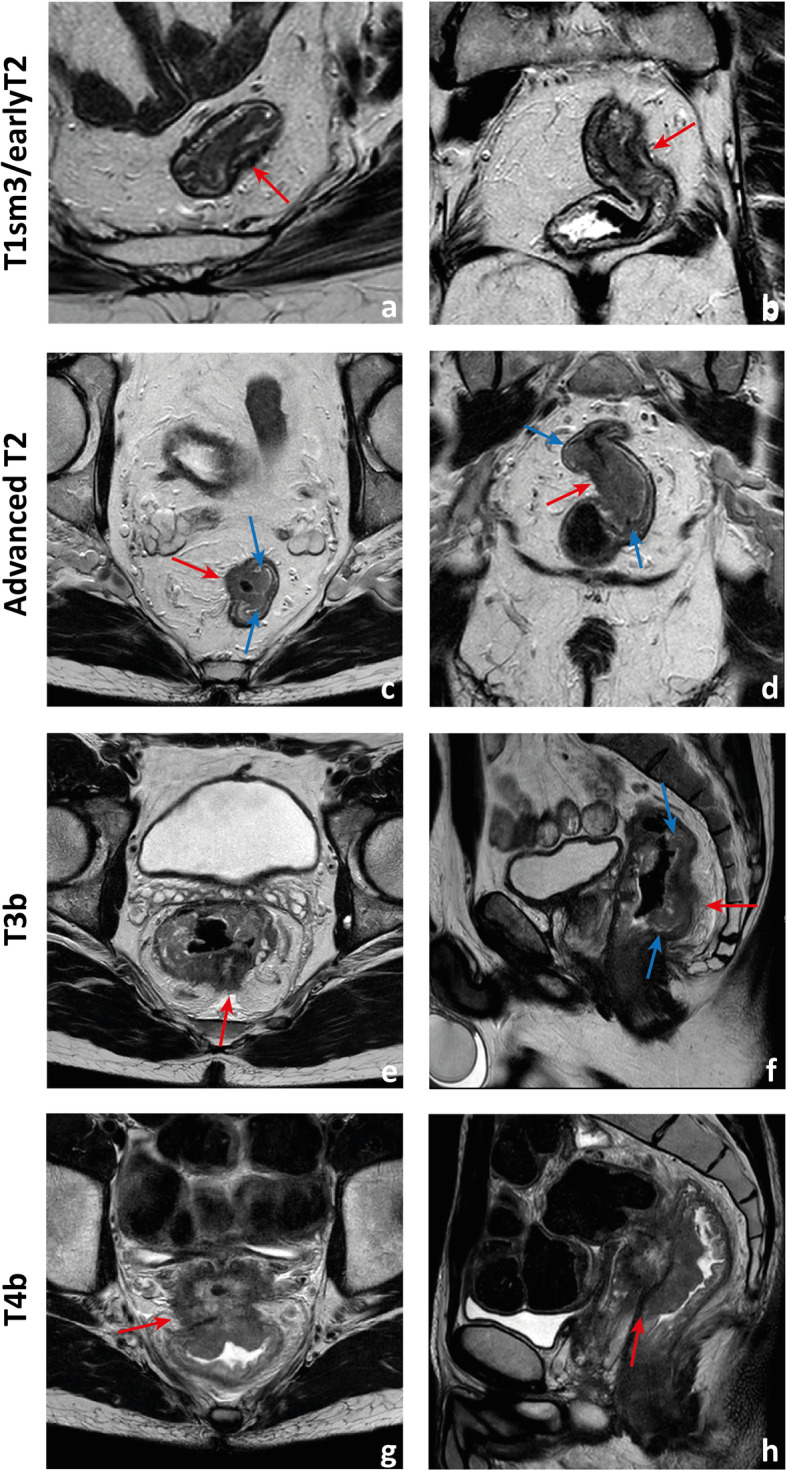
Examples of differently T-staged tumours. a, b Arrows point to an early polypoid tumour occupying the full depth of the submucosa centrally and therefore staged clinically as mrT1sm3/early T2. Total mesorectal excision was performed, and at pathology, it corresponded to a T1sm3. c, d This ulcerated tumour extends in depth through the full thickness of the muscularis propria and was therefore staged as an MR advanced T2 (red arrows), which was confirmed at pathology. Notice how the periphery of the tumour overhangs the rectal wall both in the axial and coronal planes (blue arrows). e, f This mid-high, sub-circumferential rectal cancer extends 4 mm into the mesorectal fat at its most central area (red arrows) and was therefore staged as T3b. Notice the overhanging edges on the sagittal plane (blue arrows in f). g, h An anterior mid-high rectal cancer crosses the Denonvillier fascia and the peritoneal reflection to invade the seminal vesicles in this male patient, corresponding to an mrT4b. The patient underwent chemoradiation and is currently under palliative treatment due to distant metastatic disease