
Fig 1.
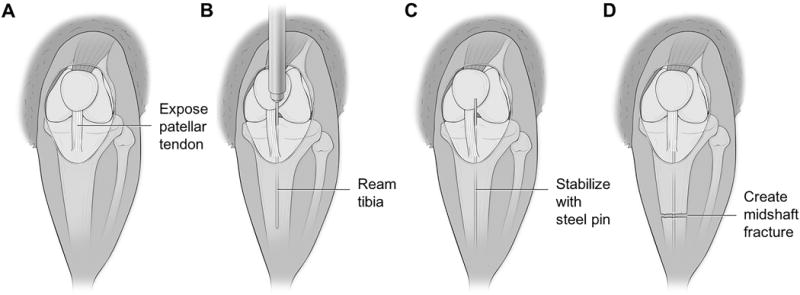
Anatomic illustrations depicting the surgical creation of the midshaft tibial fracture. (A) Illustration of right lower extremity of Sprague Dawley rat. A small midline incision was made through the skin distal to the knee joint. Skin was manually retracted towards the knee joint, exposing the patellar tendon. (B) Patellar tendon was displaced medially using forceps to expose tibial plateau. A 20gauge needle was used to ream through the tibial plateau and into the intramedullary canal. Needle was reamed distally through the canal for the entire length of the needle. (C) Reaming needle removed from canal and replaced with steel insect pin. The insect pin was inserted to the level where resistance was met. (D) Skin retracted distally to expose midshaft of tibia. Utilizing small bone cutters, a fracture was created through both cortices of the diaphyseal bone, however care was taken not to damage the intramedullary stabilizing pin. Skin again retracted proximally so the steel pin could be trimmed flush with the tibial plateau and clear from the knee joint.