
Fig. 1.
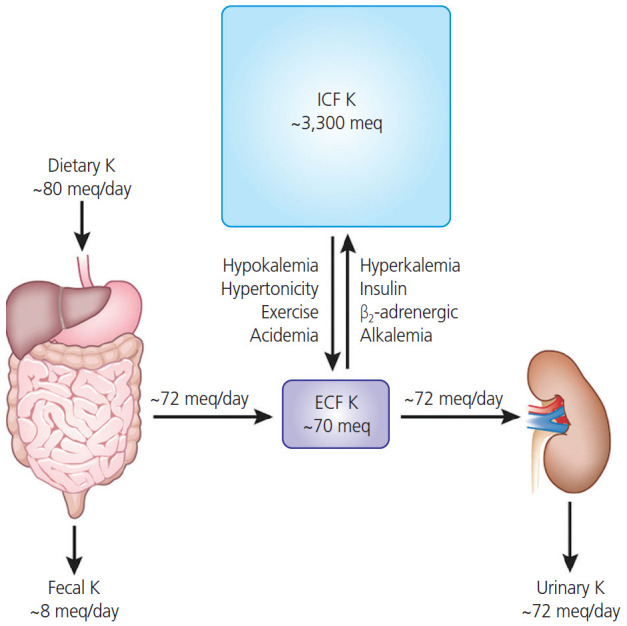
The amounts of potassium of daily dietary intake, distribution in intracellular fluid (ICF) and extracelluler fluid (ECF), and daily fecal and urinary excretion. Most dietary potassium is excreted by the kidney (up to 80 mEq/day intake vs. up to 72 mEq/day in the urine) to maintain normal potassium concentrations. Approximately 98% of potassium is present in the ICF (up to 3,300 mEq), while the other 2% present in the extracellular compartment (up to 70 mEq) which is usually maintained within a narrow range (3.8–4.5 mEq/L) in serum. Hypokalemia has many causes including: excessive potassium loss due to diarrhea, excessive sweating from exercise, abuse of alcohol, some diuretics, or laxatives. In contrast, hyperkalemia can be occurred due to acute kidney failure, chronic kidney disease, medication such as angiotensin II receptor blockers, angiotensin-converting enzyme inhibitors, or beta blockers, and dehydration or excessive potassium supplements.