

Key Points
Question
What is the cytoprotective role of neuropeptide α-melanocyte–stimulating hormone (α-MSH) treatment in preventing corneal endothelial cell loss in cold-stored human corneas under oxidative and inflammatory cytokine-induced stress?
Findings
In this comparative research study including 16 pairs of research-grade human donor corneas, α-MSH protected corneal endothelial cells from oxidative stress and inflammatory cytokine-induced cell loss in eye bank cold-stored donor corneas.
Meaning
These data suggest that supplementation of corneal storage solution with α-MSH may positively affect corneal endothelial cell survival after transplant and protect the endothelium from proinflammatory cytokines and oxidative stress after full-thickness or endothelial keratoplasty, which is particularly valuable in patients at high risk of graft failure.
This comparative research study evaluates the cytoprotective role of neuropeptide α-melanocyte–stimulating hormone treatment in preventing corneal endothelial cell loss in eye bank cold-stored corneas under oxidative and inflammatory cytokine-induced stress.
Abstract
Importance
Corneal endothelial cell (CEnC) damage and loss are major issues in eye banking and transplantation. The underlying mechanisms for CEnC loss are incompletely understood, and cytoprotective strategies that enhance CEnC viability could have a major effect on donor tissue quality and graft survival.
Objective
To investigate the cytoprotective role of neuropeptide α-melanocyte–stimulating hormone (α-MSH) in preventing CEnC loss in eye bank cold-stored corneas under oxidative and inflammatory cytokine-induced stress.
Design, Setting, and Participants
This single-center comparative research study conducted ex vivo experiments using 16 pairs of research-grade human donor corneas (courtesy of Eversight Eye Bank). Data were collected from June 2018 to November 2019, and data were analyzed from December 2019 to January 2020.
Exposures
Two corneas from the same donor were randomized to either control or 0.1 mmol/L of α-MSH treatment and then subjected to oxidative stress (1.4 mmol/L of hydrogen peroxide–phosphate-buffered saline for 15 minutes at 37 °C; n = 8 pairs) or cytokine-induced stress (100 ng/mL of tumor necrosis factor-α and 100 ng/mL of interferon γ for 18 hours at 37 °C; n = 8 pairs). Corneas were then stored at 4 °C. Specular images were taken at baseline and repeated twice per week using a calibrated wide-field specular microscope. CEnC viability was assessed using a fluorescent live/dead viability assay.
Main Outcome and Measures
Endothelial morphometry analysis, central corneal thickness measurements, and percentage of dead cells at day 11.
Results
Of 16 donors who provided corneas, 9 (56%) were male, and the mean (SD) age was 57.9 (12.4) years. Corneas were paired, and baseline parameters were comparable between all groups. At all time points, CEnC loss was lower in the α-MSH groups compared with the control groups. This difference was statistically significant after cytokine-induced stress (20.2% vs 35.2%; sample estimate of median, −14.9; 95% CI, −23.6 to −6.3; P = .008). Compared with the control group, α-MSH treatment resulted in a smaller increase in central corneal thickness (cytokine-induced stress: 89.3 μm vs 169.8 μm; sample estimate of median, −84.9; 95% CI, −131.5 to −41.6; P = .008; oxidative stress: 43.6 μm vs 111.9 μm; sample estimate of median, −68.8; 95% CI, −100.0 to −34.5; P = .008) and a smaller proportion of cell death (cytokine-induced stress: 2.7% vs 10.4%; difference, −7.7; 95% CI, −13.1 to −2.4; P = .01; oxidative stress: 2.9% vs 12.4%; difference, 9.5; 95% CI, 5.1 to 13.9; P = .006).
Conclusions and Relevance
In this study, α-MSH treatment attenuated CEnC loss during cold storage after acute oxidative and cytokine-induced stress in human eye bank cold-stored corneas. These data suggest that supplementation of corneal storage solution with α-MSH may positively affect CEnC survival after transplant and protect the endothelium from proinflammatory cytokines and oxidative stress after full-thickness or endothelial keratoplasty, which is particularly valuable in patients at high risk of graft failure.
Introduction
Corneal endothelial cell (CEnC) damage and loss are major issues in eye banking and transplantation. After full-thickness or endothelial keratoplasty, the rate of CEnC loss far exceeds that seen with normal aging,1 and donor CEnC death, whether immune driven or not,2 represents the chief proximate cause of graft failure. Although CEnC loss is known to be far more pronounced after transplant, CEnC loss may also occur during donor tissue preservation.3 In the recent Cornea Preservation Time Study,4 longer preservation times (cold storage), lower screening endothelial cell density (ECD), and donor diabetes status were all associated with significantly lower ECD at 3 years after Descemet stripping automated endothelial keratoplasty. Recent clinical evidence suggests that corneal nerve damage is associated with CEnC loss,5 implicating a role for nerve-derived factors in maintaining CEnC survival. Thus, cytoprotective strategies that enhance CEnC viability could have a major effect on donor tissue quality and graft survival. We previously found robust expression of the high-affinity melanocortin receptor (MCR) 1 for α-melanocyte–stimulating hormone (α-MSH) on CEnC in both human and murine corneas. α-MSH is a neuropeptide found in the aqueous humor, which exerts its protective and anti-inflammatory effects via the MCR family.6 In this study, we sought to investigate the cytoprotective role of α-MSH in preventing CEnC loss under oxidative and inflammatory cytokine-induced stress, the most important mediators of apoptosis during immune rejection encountered in vivo after transplant,2 using a human donor cornea tissue model.
Methods
Ex vivo experiments were conducted using 16 pairs of research-grade human donor corneas preserved in Optisol-GS cold storage solution (Bausch & Lomb). Donor cornea demographic data are summarized in the Table. Both corneas of each pair had intact epithelium, endothelium without confluent central guttae, and central ECD greater than 2000 cells/mm2 prior to testing. High-quality corneal tissue for research was courtesy of Eversight Eye Bank, Cleveland, Ohio. This experimental study adhered to the tenets of Declaration of Helsinki and The Eye Bank Association of America standards. Although hypothermic preservation represents clinically relevant CEnC stress by itself,4,7 previous in vitro experiments conducted by us and others have shown very low ECD decline in Optisol-GS cold-stored corneas.8,9 Thus, to increase the power of our study, the cytoprotective effect of α-MSH on CEnC loss in eye bank cold-stored corneas was evaluated in a controlled research environment using proinflammatory cytokines (protocol 1) and oxidative stress (protocol 2) to produce an adequate degree of CEnC injury based on previous reports.10,11 Both protocols are summarized in detail in Figure 1. In brief, corneas from each donor pair were randomized to either control (standard Optisol-GS storage solution) or α-MSH treatment (Optisol-GS supplemented with 0.1 mmol/L of α-MSH) and were subjected to either cytokine-induced stress (100 ng/mL of tumor necrosis factor [TNF]-α and 100 ng/mL of interferon [IFN] γ for 18 hours at 37 °C; n = 8 pairs)10 or oxidative stress (1.4 mmol/L of hydrogen peroxide–phosphate-buffered saline for 15 minutes at 37 °C; n = 8 pairs).11 Corneas were then stored at 4 °C (cold storage) up to 11 days. Specular images of the central corneal endothelium were taken and analyzed in a masked fashion at baseline and repeated twice per week using a calibrated wide-field specular microscope (CD-15/CellChekD+; Konan Medical) as previously reported, evaluating all corneal layers.8 A fluorescent live/dead viability assay (calcein AM–ethidium homodimer; LIVE/DEAD Viability/Cytotoxicity Kit; ThermoFisher Scientific) was used at day 11 to measure the percentage of dead cells. Statistical analysis was performed using GraphPad Prism software version 5.00 for Windows (GraphPad Software), and statistical significance was defined as P < .05. Nonparametric (paired) Wilcoxon signed rank test and 2-tailed paired t test were used for analyses.
Table. Paired Human Donor Cornea Information.
| Characteristic | Cytokine-induced stress | Oxidative stress |
|---|---|---|
| Cornea pairs, No. | 8 | 8 |
| Age, mean (SD), y | 59 (14) | 57 (11) |
| Sex, No. | ||
| Male | 5 | 4 |
| Female | 3 | 4 |
| Diabetes, No. | 5 | 3 |
| Time from death to preservation, median (range), h | 11.43 (7.63-21.25) | 11.63 (5.52-18.40) |
| Time from preservation to experiment, median (range), d | 6 (2-8) | 6 (5-8) |
| Baseline ECD, mean (SD), cells/mm2 | ||
| Control | 2681 (407) | 2796 (401) |
| α-MSH | 2583 (261) | 2839 (443) |
| P valuea | .31 | .25 |
| Baseline CV, mean (SD) | ||
| Control | 38 (3) | 33 (4) |
| α-MSH | 38 (4) | 35 (5) |
| P valuea | .44 | .20 |
| Baseline percentage of hexagonal cells, mean (SD), % | ||
| Control | 56 (3) | 59 (5) |
| α-MSH | 56 (5) | 60 (4) |
| P valuea | .73 | .80 |
| Baseline CCT, mean (SD), μm | ||
| Control | 533 (32) | 546 (42) |
| α-MSH | 529 (42) | 556 (37) |
| P valuea | .99 | .09 |
Abbreviations: CCT, central corneal thickness; CV, coefficient of variation; ECD, endothelial cell density.
Wilcoxon signed rank test (paired nonparametric test).
Figure 1. Flowcharts of the Experimental Designs for Cytokine-Induced Stress and Oxidative Stress Leading to Endothelial Damage.

Corneas from each donor pair were randomized to either control (standard Optisol-GS storage solution) or α-melanocyte–stimulating hormone (α-MSH) treatment (Optisol-GS supplemented with 0.1 mmol/L of α-MSH) and were subjected to either cytokine-induced stress (100 ng/mL of tumor necrosis factor [TNF]-α and 100 ng/mL interferon [IFN] γ for 18 hours at 37 °C; n = 8 pairs) or oxidative stress (1.4 mmol/L of hydrogen peroxide–phosphate-buffered saline for 15 minutes at 37 °C; n = 8 pairs). Corneas were then stored at 4 °C up to 11 days.
Results
Of 16 donors who provided corneas, 9 (56%) were male, and the mean (SD) age was 57.9 (12.4) years. Corneas were paired, and there was no difference in baseline morphometric parameters between corneas in the control and α-MSH groups (Table). Figure 2 summarizes the measured endothelial morphometry changes from baseline to day 7 after stress induction. CEnC loss was lower in the α-MSH groups; this difference was statistically significant after cytokine-induced stress (20.2% vs 35.2%; sample estimate of median, −14.9; 95% CI, −23.6 to −6.3; P = .008). Similarly, compared with the control groups, α-MSH treatment resulted in less pronounced changes in endothelial cell shape and significantly less corneal edema (cytokine-induced stress: 89.3 μm vs 169.8 μm; sample estimate of median, −84.9; 95% CI, −131.5 to −41.6; P = .008; oxidative stress: 43.6 μm vs 111.9 μm; sample estimate of median, −68.8; 95% CI, −100.0 to −34.5; P = .008), suggesting that CEnC function might be better preserved with α-MSH treatment. Specular images are shown in eFigure 1 in the Supplement. This was confirmed with immunohistochemistry, as a significantly lower percentage of dead cells were observed in the α-MSH groups compared with the control groups (cytokine-induced stress: 2.7% vs 10.4%; difference, −7.7; 95% CI, −13.1 to −2.4; P = .01; oxidative stress: 2.9% vs 12.4%; difference, 9.5; 95% CI, 5.1 to 13.9; P = .006) (eFigures 2 and 3 in the Supplement).
Figure 2. Change in Endothelial Morphometry and Cell Death During Hypothermic Storage Under Cytokine-Induced or Oxidative Stress.
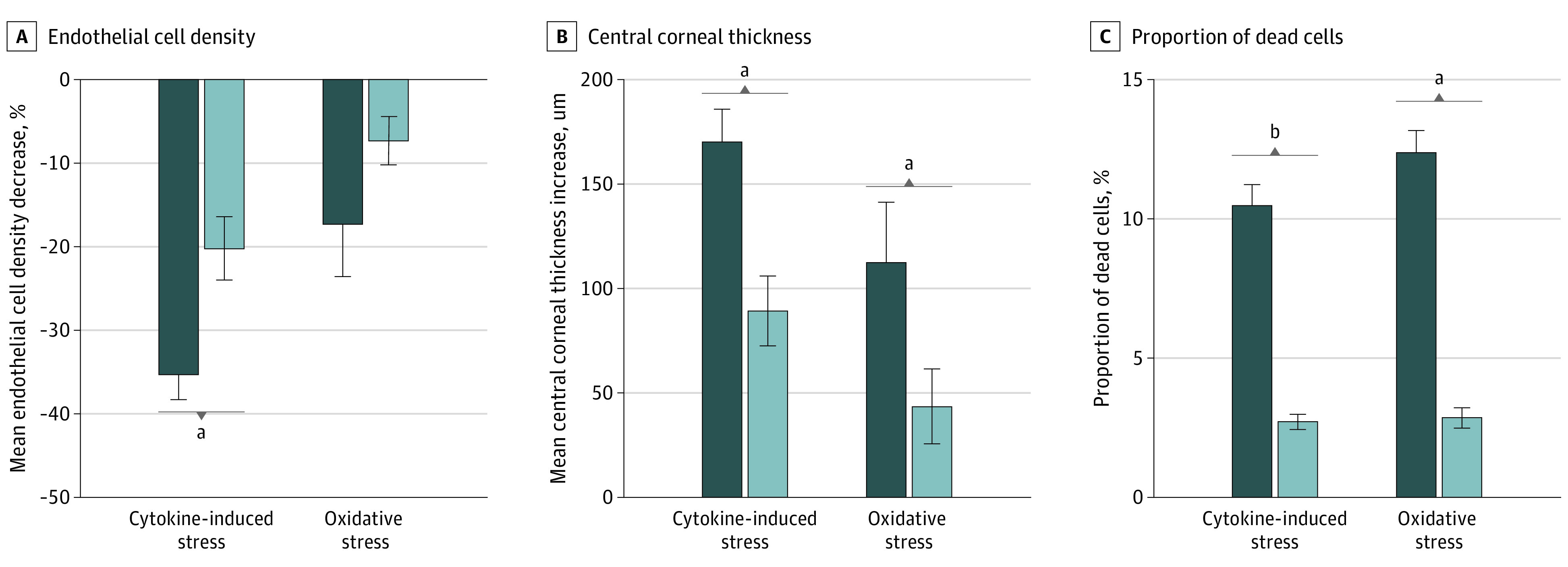
A, The calculated mean percentage of endothelial cell density decline was lower in the α-melanocyte–stimulating hormone (α-MSH) treatment group compared with the control group. B, The mean increase in central corneal thickness was lower in the α-MSH group compared with the control group. C, Bar diagram showing a significantly lower percentage of dead cells (ethidium homodimer I–positive) in the α-MSH groups compared with the control groups. Error bars indicate the standard error of the mean.
aP < .01.
bP < .05.
Discussion
Multiple extracellular and cellular stressors induce CEnC loss in donor corneal tissue procurement and storage and after transplant. Previous studies have shown apoptosis of CEnC during immune rejection is most likely propagated by the synergistic effect of proinflammatory cytokines, including TNF-α and IFN-γ, and oxidative stress (hydrogen peroxide that is produced by immune cells).2 TNF-α and IFN-γ play a major role in corneal endothelial dysfunction during allograft rejection, and elevated levels of these cytokines have also been identified in the aqueous humor of patients with bullous keratopathy or low ECD.12
These data suggest that supplementation of corneal storage solution with α-MSH may positively affect CEnC survival after transplant and protect the endothelium from proinflammatory cytokines after full-thickness or endothelial keratoplasty. The latter may prove to be particularly valuable in patients at high risk of graft failure, such as those with a history of glaucoma or previous graft rejection.
Limitations
Our study was limited by a small sample size, as high-quality donor corneas are preserved for transplant, and availability for research use is limited. We sought to overcome the sample size issue with high-quality paired tissues and a rigorous experimental design. Gradual decline in specular image quality associated with longer storage times and corneal epithelial changes (eg, epithelial defects) can lead to artifacts and inaccurate measurements; we therefore performed masked observation, evaluating all corneal layers, and performed live/dead cell assay using immunohistochemistry to confirm specular findings. In addition, all parameters recorded using specular microscopy demonstrated similar trends.
Conclusions
In summary, the present study demonstrates that α-MSH supplementation of cold-storage solution protects the corneal endothelium from oxidative stress and proinflammatory cytokines. Future studies examining the cytoprotective role of α-MSH in prolonging hypothermic tissue storage (extended preservation) and in preserving CEnC after endothelial graft preparation (preloaded tissue) by eye banks prior to transplant are warranted.
eFigure 1. Representative specular microscopy images in the control and α-MSH groups.
eFigure 2. Immunofluorescence images in the control and α-MSH group under oxidative stress.
eFigure 3. Immunofluorescence images in the control and α-MSH group under inflammatory cytokine-induced stress.
References
- 1.Nishimura JK, Hodge DO, Bourne WM. Initial endothelial cell density and chronic endothelial cell loss rate in corneal transplants with late endothelial failure. Ophthalmology. 1999;106(10):1962-1965. doi: 10.1016/S0161-6420(99)90409-8 [DOI] [PubMed] [Google Scholar]
- 2.Chauhan SK, Jurkunas U, Funaki T, Dastjerdi M, Dana R. Quantification of allospecific and nonspecific corneal endothelial cell damage after corneal transplantation. Eye (Lond). 2015;29(1):136-144. doi: 10.1038/eye.2014.248 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kitazawa K, Inatomi T, Tanioka H, et al. The existence of dead cells in donor corneal endothelium preserved with storage media. Br J Ophthalmol. 2017;101(12):1725-1730. doi: 10.1136/bjophthalmol-2017-310913 [DOI] [PubMed] [Google Scholar]
- 4.Lass JH, Benetz BA, Patel SV, et al. ; Cornea Preservation Time Study Group . Donor, recipient, and operative factors associated with increased endothelial cell loss in the cornea preservation time study. JAMA Ophthalmol. 2019;137(2):185-193. doi: 10.1001/jamaophthalmol.2018.5669 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lambiase A, Sacchetti M, Mastropasqua A, Bonini S. Corneal changes in neurosurgically induced neurotrophic keratitis. JAMA Ophthalmol. 2013;131(12):1547-1553. doi: 10.1001/jamaophthalmol.2013.5064 [DOI] [PubMed] [Google Scholar]
- 6.Clemson CM, Yost J, Taylor AW. The role of alpha-MSH as a modulator of ocular immunobiology exemplifies mechanistic differences between melanocortins and steroids. Ocul Immunol Inflamm. 2017;25(2):179-189. doi: 10.3109/09273948.2015.1092560 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jeng BH, Meisler DM, Hollyfield JG, Connor JT, Aulak KS, Stuehr DJ. Nitric oxide generated by corneas in corneal storage media. Cornea. 2002;21(4):410-414. doi: 10.1097/00003226-200205000-00015 [DOI] [PubMed] [Google Scholar]
- 8.Lužnik Z, Sun Z, Yin J, Benetz BA, Lass JH, Dana R. A standardized methodology for longitudinal assessment of corneal endothelial morphometry in eye banked corneas. J Biol Methods. 2019;6(4):e120-e120. doi: 10.14440/jbm.2019.304 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Means TL, Geroski DH, Hadley A, Lynn MJ, Edelhauser HF. Viability of human corneal endothelium following Optisol-GS storage. Arch Ophthalmol. 1995;113(6):805-809. doi: 10.1001/archopht.1995.01100060131047 [DOI] [PubMed] [Google Scholar]
- 10.Coco G, Foulsham W, Nakao T, et al. Regulatory T cells promote corneal endothelial cell survival following transplantation via interleukin-10. Am J Transplant. 2020;20(2):389-398. doi: 10.1111/ajt.15631 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Koh SWM, Waschek JA. Corneal endothelial cell survival in organ cultures under acute oxidative stress: effect of VIP. Invest Ophthalmol Vis Sci. 2000;41(13):4085-4092. [PubMed] [Google Scholar]
- 12.Yamaguchi T, Higa K, Suzuki T, et al. Elevated cytokine levels in the aqueous humor of eyes with bullous keratopathy and low endothelial cell density. Invest Ophthalmol Vis Sci. 2016;57(14):5954-5962. doi: 10.1167/iovs.16-20187 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eFigure 1. Representative specular microscopy images in the control and α-MSH groups.
eFigure 2. Immunofluorescence images in the control and α-MSH group under oxidative stress.
eFigure 3. Immunofluorescence images in the control and α-MSH group under inflammatory cytokine-induced stress.