

Abstract
Background and study aims The quality of screening-related colonoscopy depends on several physician- and patient-related factors. Adenoma detection rate (ADR) varies considerably between endoscopists. Educational interventions aim to improve endoscopists’ ADRs, but their overall impact is uncertain. We aimed to assess whether there is an association between educational interventions and colonoscopy quality indicators.
Methods A comprehensive search was performed through August 2019 for studies reporting any associations between educational interventions and any colonoscopy quality indicators. Our primary outcome of interest was ADR. Two authors assessed eligibility criteria and extracted data independently. Risk of bias was also assessed for included studies. Pooled rate ratios (RR) with 95 % confidence intervals (CI) were reported using DerSimonian and Laird random effects models.
Results From 2,253 initial studies, eight were included in the meta-analysis for ADR, representing 86,008 colonoscopies. Educational interventions were associated with improvements in overall ADR (RR 1.29, 95 % CI 1.25 to 1.42, 95 % prediction interval 1.09 to 1.53) and proximal ADR (RR 1.39, 95 % CI 1.29 to 1.48), with borderline increases in withdrawal time, ([WT], mean difference 0.29 minutes, 95 % CI – 0.12 to 0.70 minutes). Educational interventions did not affect cecal intubation rate ([CIR], RR 1.01, 95 % CI 1.00 to 1.01). Heterogeneity was considerable across many of the analyses.
Conclusions Educational interventions are associated with significant improvements in ADR, in particular, proximal ADR, and are not associated with improvements in WT or CIR. Educational interventions should be considered an important option in quality improvement programs aiming to optimize the performance of screening-related colonoscopy.
Introduction
In 2020, it is estimated that nearly 150,000 individuals will be newly diagnosed with colorectal cancer (CRC) in the United States alone, with over 50,000 expected CRC-related deaths 1 . CRC is a disease process that is appropriate for employing population-based screening, given that its natural history typically involves a slow progression from adenoma to cancer 2 . Colonoscopy has been shown to reduce CRC incidence and mortality in a cost-effective fashion 3 4 , given its capacity to both identify and remove adenomatous polyps. It can thus potentially act either as a primary screening modality or a primary method of following up on other abnormal screening tests.
To assess and optimize the overall quality of screening-related colonoscopy, several surrogate indicators have been widely adopted, including cecal intubation rate (CIR) and adenoma detection rate (ADR) 5 6 . There is a well-established relationship between higher ADR and lower incidence of post-colonoscopy CRC (PCCRC) 7 . Rates of PCCRC can vary depending on the methodology used for their calculation, but are thought to range from 3 % to 13 % with an estimated average of 7.4 % 8 9 . Several screening programs mandate minimum ADR benchmarks of ≥ 25 % for screening colonoscopy 5 10 , with some advocating for higher targets depending on the population(s) being screened 11 .
Despite efforts to improve colonoscopy quality, wide variations in endoscopists’ ADRs exist 12 13 14 . Suboptimal technique and inadequate withdrawal times (WTs) are considered to be major factors responsible for this disparity 15 . Several interventions have been studied that aim to improve ADR, ranging from medical devices 16 to optimized endoscopy curricula for trainees 17 . Of particular interest are educational interventions specifically targeted at independently practicing endoscopists. Despite planned systematic performance improvement interventions 18 , early evidence failed to demonstrate significant improvements in ADR, leading some to conclude that educational interventions do not improve colonoscopy quality. However, more recent evidence reported that the implementation of a bundle of educational interventions was associated with significant ADR improvements in the poorest performers 19 .
We performed a systematic review and meta-analysis to determine whether there is an association between educational interventions and improvements in ADR or any other colonoscopy quality indicators.
Methods
Overview
Our systematic review was conducted and reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement recommendations 20 and Meta-analysis of Observational Studies in Epidemiology (MOOSE) statement recommendations. A detailed PRISMA checklist is provided in Supplementary Table 1 . The protocol for this review was registered on PROSPERO (CRD42019149683). Our primary objective was to determine if there is an association between educational interventions for endoscopists and improvement in ADR. Our secondary objectives were to evaluate whether endoscopist educational interventions are associated with improvements in other colonoscopy quality indicators: polyp detection rate (PDR), advanced neoplasm detection rate (ANDR), proximal ADR (pADR), CIR and WT.
Search strategy
A comprehensive search strategy was developed by members of the study team in conjunction with a health research librarian. We searched MEDLINE, EMBASE (Excerpta Medica Database), Google Scholar, and CENTRAL (Cochrane Central Registry of Controlled Trials) from inception of the databases through August 31, 2019. Our full search strategy is provided along with additional gray literature searches performed in Appendix 1 .
Eligibility criteria
A study was eligible for inclusion if it was a cohort study, quasi-experimental study or clinical trial, it was published in English as either an abstract or manuscript, it assessed the effect of an educational intervention targeting colonoscopy (including live lectures, slide decks, video tutorials, online training modules, individualized assessment and optimization, and skills enhancement and training courses), and it reported on at least one colonoscopy quality indictor (including ADR, PDR, ANDR, pADR, CIR, or WT).
A study was excluded if it reported on data that overlapped with another published study, in part or in whole (in these cases, the study with longer follow up or more complete data was included), it assessed the effect of educational interventions on the performance of trainees, or it assessed only the effect of audit and feedback or other interventions without a targeted educational intervention.
Study selection
Following removal of duplicates, citations were imported into Rayyan (M Ouzzani, Qatar Computing Research Institute, HBKU, Doha, Qatar). All abstracts were screened independently by two reviewers (EGM, KB). In the case of disagreements, a third author (NF) reviewed the study and consensus was achieved. The full-length texts of selected abstracts were retrieved and reviewed.
Data extraction and study quality
A data abstraction form was designed a priori to collect data from each included study. Two reviewers (EGM, KB) independently extracted pre-established data points, in addition to performing assessments of bias and overall study quality. The risk of bias in individual studies was determined using the Newcastle-Ottawa Scale (NOS) for non-randomized studies 21 . Inter-reviewer discrepancies in data abstraction were resolved by consensus after input of a third author (NF). When studies met inclusion criteria but had insufficient data to be included in the quantitative meta-analysis, we attempted to contact corresponding authors to obtain missing information; if unsuccessful, the study was summarized qualitatively only. We used the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) system to assess the certainty of the evidence according to study design, consistency, directness, imprecision and reporting bias 22 .
Outcomes
The primary outcome of our study was ADR. Secondary outcomes of interest were PDR, ANDR, pADR, WT and CIR.
Statistical analysis
Rate ratios (RR) with their respective 95 % confidence intervals (CI) were pooled and presented in Forest plots to estimate the effect of educational interventions on outcomes. Whenever a randomized controlled trial (RCT) also presented preintervention and post-intervention data, we: a) pooled these data along with the meta-analysis of other quasi-experimental observational studies; and b) analyzed the randomized data separately. We defined RR as the ratio of the post-intervention quality indicator divided by the pre-intervention value. For continuous variables such as WT, we calculated mean differences in preintervention and post-intervention measures. We used DerSimonian and Laird random effects models to account for expected heterogeneity across study designs. In addition, the 95 % prediction interval for the primary outcome of interest was calculated 23 . χ 2 tests and I 2 statistics were calculated as a measure of between study heterogeneity. I 2 values of 0 – 30 % were regarded as possibly unimportant, values of 30 % to 50 % were regarded to represent moderate heterogeneity, values of 50 % to 75 % were regarded to represent substantial heterogeneity, and values > 75 % were regarded to represent considerable heterogeneity 24 . Funnel plots as well as Egger’s and Begg’s tests were used to assess publication bias 25 26 .
To assess other potential sources of heterogeneity, we performed several subgroup analyses, including by study design (RCTs versus observational studies), number of centers (single-center versus multicenter), and publication type (conference abstract versus published manuscript). Subgroup analyses were also performed by indication for colonoscopy (primarily screening-related versus mixed populations), education type (hands-on versus didactic training programs), Endoscopic Quality Improvement Program (EQUIP)-based 27 versus other strategies, and presence of lag time (any versus none). Lag time was defined as any time period between the intervention and outcome measurement. Meta-regression analyses were not performed given that there were fewer than 10 studies in the analysis for the primary outcome 24 .
We conducted sensitivity analyses whereby each study was removed in turn and whereby fixed effects models were used rather than random effects models. Statistical analyses were performed using STATA version 14.2 (StataCorp, College Station, Texas, United States) and Revman 5.3 (Cochrane Collaboration).
Results
Study selection
A PRISMA flowchart summarizing the overall search results and study selection process is presented in Supplementary Fig. 1 . A total of 2,253 citations were identified from the search strategy, without any additional studies identified through manual searches. Of these, 30 full-text articles were reviewed. Eight studies were included in the meta-analysis for the primary outcome. An additional two studies did not contain sufficient data to be quantitatively analyzed despite attempts to contact study authors; thus, these were summarized qualitatively.
Study characteristics and quality
Baseline characteristics of the studies included in the meta-analysis are summarized in Table 1 . Seven studies were performed in North America and one was performed in Europe. Included studies were published between 2010 and 2019. Three were RCTs 27 28 29 , four employed quasi-experimental designs (pre-comparisons and post-comparisons) 30 31 32 33 and one was a retrospective cohort with pre-comparisons and post-comparisons 34 . A summary of interventions and outcomes from studies included in the meta-analysis is provided in Table 2 .
Table 1. Summary of characteristics of studies included in the meta-analysis.
| Author, year |
Study type | Country | Number of study sites | Endoscopists (N = ), specialty, practice type | Colonoscopies (N = ) pre-/post- intervention | Patient sex (% male) | Median patient age | Indication (% screening-related) | Study quality |
| Berger 2017 33 | OBS | USA | 1 | 11, 100 % GI, academic | 1,113/849 | N/R | N/R | N/R | N/A * |
| Coe 2013 27 | RCT | USA | 1 | 15, 100 % GI, academic | 602/520 | 51 | 63 | 42 | NOS-8 |
| Corley 2019 32 | OBS | USA | 20 | 85, specialty N/R, setting N/R | 12,266/20,897 | 49 | 63 | 22 | N/A * |
| Evans 2019 34 | OBS | Canada | 1 | 14, specialty N/R, academic | 833/850 | ||||
| Hall 2010 31 | OBS | USA | 1 | 11, 100 % GI, academic | 550/413 | 48 | 53 | 100 | N/A * |
| Kaminski 2016 29 | RCT | Poland | 38 | 38, specialty N/R, setting: National CRC Screening Program | 14,264/10,615 | 39 | 57 | 100 | NOS-9 |
| Keswani 2015 30 | OBS | USA | 1 | 20, specialty N/R, setting N/R | 2,444/3,639 | N/R | N/R | 100 | NOS-8 |
| Wallace 2017 28 | RCT | USA | 9 | N/R | 7,480/8,673 | 59 | 47 | 70 | NOS-8 |
OBS, observational study; RCT, randomized controlled trial; GI, gastroenterologist; Sx, surgeon; NOS, Newcastle-Ottawa Scale 21 ; N/R = not reported
conference abstract.
Table 2. Summary of interventions and outcomes from studies included in the meta-analysis.
| Author, year | Description of educational intervention | Number of sessions | Lag time after intervention * | Post-intervention observation period | Preintervention ADR | Post-intervention ADR | Other outcomes reported |
| Berger 2017 33 | One-hour slide show presentation/ lecture -focusing on improving ADR (EQUIP I/II intervention). | One | None | N/R | 33.0 | 41.9 | PDR, SPDR |
| Coe 2013 27 | EQUIP I: two slide show presentations that included videos, images, and reference material along with pre- and post- tests (each session duration of approximately 1 hour). First session : methods and technical aspects; lesion recognition (particularly flat lesions). Second session : pre- and post-test on neoplastic vs. non-neoplastic lesions and advanced imaging modalities. | Two | 4 months | 7 months | 36.0 | 47.0 | PDR, ANDR, pADR |
| Corley 2019 32 | 30-minute interactive online training module on polyp identification, cleaning/washing techniques, and colonoscopy quality, combined with feedback on ADR. | One | None | 24 months | 31.5 | 37.4 | None |
| Evans 2019 34 | Colonoscopy Skills Improvement (CSI) program, consisting of one day live endoscopy sessions, with two certified faculty teaching up to three 3 endoscopists per session. | One | None | 8 months | 31.8 | 35.3 | WT, CIR |
| Hall 2010 31 | Departmental education regarding current national recommendations regarding withdrawal times and expected detection rates. | One | 28 months | 3 months | 22.0 | 34.0 | WT |
| Kaminski 2016 29 | Train-Colonoscopy-Leaders (TCL) cours, comprising three phases. Phase I : a 2-hour assessment visit by endoscopy nurses (10 colonoscopies) and two-day training by UK trainers (skills improvement, training the trainer, leadership training). Phase II: 2-day hands on training. Phase III: repeat previous nurse assessments (10 colonoscopies); evaluation of first 30 colonoscopies with feedback. | Two | None | 18 months | 18.4 | 24.1 | PDR, SPDR, CIR, pADR |
| Keswani 2015 30 | Physician report cards containing endoscopistsʼ and institutional ADRs and WT, as well as the institutional mean ADR and ADRs of the 10th and 90th percentile. Concurrent educational meeting detailing the data supporting ADR and its relationship with interval CRC cancer and the report card methodology. | One | 12 months | 6 months | 28.0 | 39.0 | WT |
| Wallace 2017 28 | One-hour lecture focusing on improving adenoma detection (EQUIP I/II intervention) followed by: 1 – 2-h review session, identification of low performers, discussion of obstacles to high quality colonoscopy. In addition, optional one-on-one proctoring is offered as well as telephone calls to discuss progress. EQUIP posters are posted in endoscopy units. | One | N/R | N/R | 31.0 | 42.0 | PDR, ANDR, CDR, WT |
ADR, adenoma detection rate; CIR, cecal intubation rate; WT, withdrawal time; SPDR, sessile polyp detection rate; PDR, polyp detection rate; ANDR, advanced neoplasia detection rate; pADR, proximal adenoma detection rate; N/R, not reported.
Lag time refers to time between intervention and start of post-intervention measurement of outcome(s).
Summaries of quality assessments are provided in Table 1 , with full assessments provided in Supplementary Table 2 and Supplementary Fig. 2 . Study quality was high for fully published studies, with a mean NOS of 8.25. Assessments of the certainty of the evidence according to the GRADE approach 22 are summarized in Table 3 . Summaries of studies included in the systematic review, but not quantitatively analyzed via meta-analysis, are provided in Supplementary Table 3 .
Table 3. GRADE summary of effects of feedback interventions on colonoscopy quality indicators 22 .
| Outcomes | Anticipated absolute effects 1 (95 % CI) | Relative effect (95 % CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with control | Risk with Educational interventions | |||||
| Adenoma detection rate – all studies as observational (ADR – Obs) | 265 adenomas detected per 1,000 colonoscopies | 341 per 1,000 (323 to 362) | Rate ratio 1.29 (1.22 to 1.37) | 86008 (8 observational studies) | ⊕⊕○○ LOW | Educational interventions likely result in an increase in adenoma detection rate – all studies as observational. |
| Adenoma detection rate – only non-randomized studies (ADR) | 308 adenomas detected per 1,000 colonoscopies | 391 per 1,000 (357 to 431) | Rate ratio 1.27 (1.16 to 1.40) | 43854 (5 observational studies) | ⊕○○○ VERY LOW 2 | Educational interventions may result in an increase in adenoma detection rate. |
| Adenoma detection rate – only RCTs (ADR-RCTs) | 267 adenomas detected per 1,000 | 315 per 1,000 (283 to 350) | Rate ratio 1.18 (1.06 to 1.31) | 25791 (3 RCTs) | ⊕⊕⊕○ MODERATE | Educational interventions likely increase adenoma detection rate – only RCTs. |
| Polyp Detection Rate (PDR) | 494 polyps detected per 1,000 colonoscopies | 608 per 1,000 (593 to 628) | Rate ratio 1.23 (1.20 to 1.27) | 19237 (3 observational studies) | ⊕○○○ VERY LOW 2 | Educational interventions may increase polyp detection rate but the evidence is very uncertain. |
| Proximal adenoma detection rate (pADR) | 93 proximal adenomas detected per 1,000 colonoscopies | 130 per 1,000 (120 to 138) | Rate ratio 1.39 (1.29 to 1.48) | 26001 (2 observational studies) | ⊕○○○ VERY LOW 2 | Educational interventions may increase proximal adenoma detection rate but the evidence is very uncertain. |
| Withdrawal time (WT) | The mean withdrawal time was 10.5 minutes | MD 0.29 minutes higher (0.18 lower to 0.76 higher) | – | 48393 (4 observational studies) | ⊕○○○ VERY LOW | Educational interventions may increase withdrawal time but the evidence is very uncertain. |
| Cecal intubation rate (CIR) | 962 per 1,000 colonoscopies | 962 per 1,000 (962 to 971) | Rate ratio 1.00 (1.00 to 1.01) | 26562 (2 observational studies) | ⊕○○○ VERY LOW | Educational interventions may have little to no effect on cecal intubation rate but the evidence is very uncertain. |
ADR, adenoma detection rate; RR, rate ratio; CI, confidence interval; MD, mean difference; OBS, observational studies
GRADE Working Group grades of evidence:
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect
Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different
Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect
Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect
The risk in the intervention group (and its 95 % confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 % CI).
a. All the observational studies are quasi-experimental with before and after comparisons. b. The heterogeneity, both statistical and clinical, is substantial and cannot be fully explained. c. The overlap between the confidence intervals is very limited. d. The confidence in the estimate is low (the 95 % CI for the pooled estimate is wide and/or crosses the line of no effect).
Adenoma detection rate
Meta-analysis of eight studies compared the ADR pre-education and post-education as RRs and included 86,008 colonoscopies. The pooled baseline ADR was 26.5 % and the post-intervention ADR was 35.4 %. Educational interventions were associated with a 29 % relative increase in ADR (RR 1.29, 95 % CI 1.22 to 1.37, 95 % prediction interval 1.09 to 1.53) as shown in Fig. 1 . There was considerable heterogeneity between the eight included studies, demonstrated by an I 2 value of 82.96 % ( Fig. 1 ).
Fig. 1.
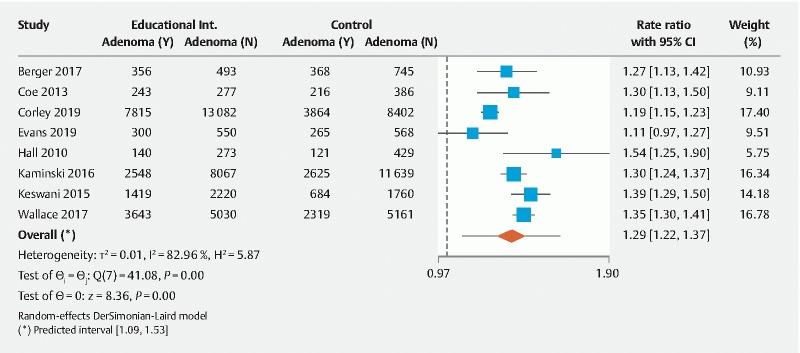
Forest plot comparing the primary outcome of adenoma detection rate (ADR) pre-educational intervention and post-educational intervention. CI, confidence interval.
Two additional studies met inclusion criteria for the primary outcome but did not contain sufficient data to be included in the meta-analysis, even after attempts to contact corresponding author(s) were made. Both studies reported significant improvements in ADR following multi-level educational interventions 35 36 .
Polyp detection rate
Three studies representing 19,237 colonoscopies compared PDR pre- and post-educational interventions. At baseline, PDR was 49.4 %, whereas after the intervention it increased to 61.1 %. We found that educational interventions were associated with a 23 % relative increase in PDR (RR 1.23, 95 % CI 1.19 to 1.27), as demonstrated in Fig. 2a . There was low heterogeneity between the included studies ( I 2 value of 11.21 %).
Fig. 2.
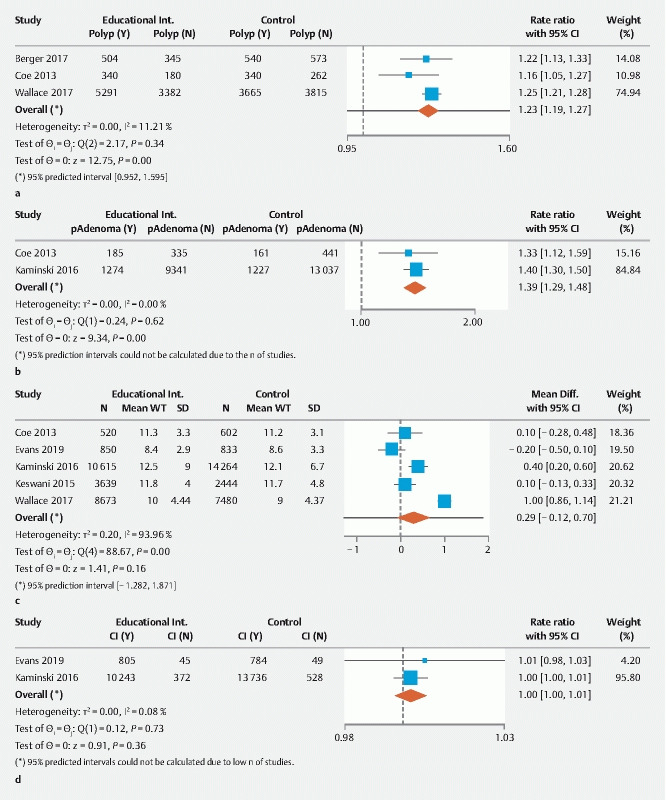
Forest plot comparing a polyp detection rate (PDR), b proximal adenoma detection rate (pADR), c withdrawal time (WT), and d cecal intubation rate (CIR) pre-educational intervention and post-educational intervention. CI, confidence interval.
Proximal adenoma detection rate
Two studies reported pADR before and after educational interventions, representing 26,001 colonoscopies. Prior to the intervention, the pADR was 9.3 %, whereas after the intervention it increased to 13.10 %. Educational interventions were associated with a 39 % relative increase in pADR (RR 1.39, 95 % CI 1.29 to 1.48) as displayed in Fig. 2b . There was no heterogeneity between the studies ( I 2 value of 0 %).
Withdrawal time
Four studies representing 50,106 colonoscopies that compared WT before and after educational interventions were included in the meta-analysis. WT was relatively homogeneously defined across studies, being either calculated using negative procedures only, or using all procedures with a timer used to remove period(s) spent on any intervention(s) performed. There were no significant differences in WT (MD 0.29 minutes, 95 % CI – 0.12 to 0.70 minutes) as shown in Fig. 2c . There was considerable heterogeneity between these studies ( I 2 value of 93.96 %). Of note, the WTs in the majority of the included studies exceeded those proposed by guidelines 5 6 , ranging from 8.6 to 12.1 minutes in the preintervention arm and from 8.4 to 12.5 minutes in the post-intervention arm.
Cecal intubation rate
Two studies reported on CIR preintervention and post-intervention, representing 25,568 colonoscopies. There were no significant changes in CIR before and after educational interventions, as shown in Fig. 2d (RR 1.00, 95 % CI 1.00 to 1.01). There was no heterogeneity between the included studies ( I 2 value of 0.08 %). Of note, the pooled CIR met recommended targets 5 6 in both the pre- and post-intervention periods, at 96.2 % and 96.4 %, respectively.
Subgroup analyses
Lag times (times between the intervention and the start of outcome measurement) were clearly reported in five studies and varied between 6 and 28 months. The improvement in ADR was slightly less pronounced in studies reporting any lag time following educational interventions compared with studies with no lag time or no lag time reported (RR 1.28, 95 % CI 1.19 to 1.38 and RR 1.34, 95 % CI 1.28 to 1.41, respectively). However, this difference was not statistically significant (p = 0.32). The first subgroup, however, had substantial inter-study heterogeneity ( I 2 82 %) whereas the second had low heterogeneity ( I 2 11 %). There were no significant differences in ADR improvements between studies in screening and mixed populations, hands-on versus didactic training programs, or EQUIP-based versus other strategies. Interestingly, heterogeneity was absent between the EQUIP-based studies ( I 2 0 %) and when randomized trials were grouped together using before-and-after data ( I 2 0 %). There were also no significant differences in subgroup analyses by study design (RCT versus observational), number of centers (single-center versus multicenter), or publication type (published manuscript versus conference abstract). The inter-study heterogeneity was slightly reduced within the subgroup containing only single-center studies ( I 2 value of 64 %), and in the subgroup containing only full text publications ( I 2 59 %). When the three RCTs were analyzed using experimental and control groups, the rate ratio was still significant (RR 1.18, 95 % CI 1.06 to 1.31), but less pronounced than when these studies were analyzed using pre-intervention and post-intervention groups in order to compare them with other observational studies (RR 1.33, 95 % CI 1.29 to 1.37). Subgroup analyses are summarized in Table 4 and are provided in detail in Supplementary Fig. 3 .
Table 4. Summary of subgroup analyses.
| Subgroups | Pooled RR (95 % CI) | Inter-study heterogeneity ( I 2 ) |
| No lag time * 28 33 34 | 1.34 (1.28, 1.41) | 11 % |
| Any lag time specified * 27 29 30 31 32 | 1.28 (1.19, 1.38) | 82 % |
| Primarily screening colonoscopy 28 29 30 31 33 | 1.32 (1.25, 1.39) | 60 % |
| Mixed populations 27 32 34 | 1.21 (1.12, 1.30) | 37 % |
| EQUIP-based studies 27 28 33 | 1.34 (1.29, 1.39) | 0 % |
| Non-EQUIP-based studies 29 30 31 32 34 | 1.28 (1.18, 1.39) | 86 % |
| Hands-on skills training 29 34 | 1.22 (1.04, 1.43) | 80 % |
| Didactic training 27 28 30 31 32 33 | 1.32 (1.22, 1.42) | 86 % |
| Published manuscripts 27 28 29 30 34 | 1.32 (1.25, 1.38) | 59 % |
| Conference abstracts 31 32 33 | 1.28 (1.14, 1.43) | 71 % |
| RCT (pre-/post-) 27 28 29 | 1.33 (1.29, 1.37) | 0 % |
| RCT (control/intervention) 27 28 29 | 1.18 (1.06, 1.31) | 82 % |
| Observational studies 30 31 32 33 34 | 1.27 (1.16, 1.40) | 82 % |
| Multi-center studies 28 29 32 | 1.28 (1.17, 1.39) | 93 % |
| Single-center studies 27 30 31 33 34 | 1.31 (1.19, 1.43) | 64 % |
RR, rate ratio of ADR post- versus preintervention; CI, confidence interval; RCT, randomized
controlled trial; EQUIP 27 , endoscopic quality improvement program.
Lag time refers to time between intervention and start of post-intervention measurement of outcome(s).
Other sensitivity analyses and publication bias
The findings for our primary outcome of ADR were robust to sensitivity analysis, as the RR did not change appreciably with exclusion of each study in turn or with analysis using a fixed effects model. There was no evidence of publication bias for the primary outcome by Egger’s or Begg’s tests, or by visual inspection of the funnel plot ( Supplementary Fig. 4 ).
Discussion
In our meta-analysis of eight studies including 86,008 colonoscopies, educational interventions were associated with a significant 29 % relative increase in ADR. We also found that educational interventions are associated with significant improvements in PDR and pADR. Other quality indicators such as WT and CIR remained unchanged after educational interventions, though there was a trend toward increases in WT. Our results suggest that educational interventions aimed at independently practicing endoscopists contribute meaningfully to improvements in colonoscopy indicators.
ADR is the most widely endorsed colonoscopy quality indicator given its established inverse relationship with PCCRC 7 and CRC-related death 37 . Various strategies to optimize ADR specifically aimed at the endoscopist have been studied, including formalized audit and feedback 38 , video-based assessments 39 40 , and combinations of these strategies 18 , with mixed results. Short educational interventions targeting endoscopists, the subject of this review, have also been studied. Though these interventions vary considerably, they have in common the ultimate goal of improving the quality of colonoscopy performed by independent non-trainee endoscopists. EQUIP training, for example, is comprised of didactic presentations focusing on optimal withdrawal techniques and image recognition of neoplastic versus non-neoplastic polyps 27 . Conversely, skills enhancement and ‘train-the-endoscopy-trainer’ programs take a more holistic approach, providing a range of theoretical and hands-on training sessions, from basic to advanced 41 . These sessions are primarily focused on navigating the transition from unconscious competence to conscious competence 42 , but also have the concurrent effect of optimizing technique and enabling more robust teaching, ultimately improving quality indicators 29 . Our findings confirm that these interventions have a demonstrable effect on several important colonoscopy quality indicators. Interestingly, studies assessing hands-on training interventions improved ADR at approximately the same rate as didactic interventions in our study. While hands-on training, including simulation, is currently recommended as part of endoscopy training curricula 43 , its use among trained endoscopists has been relatively poorly studied.
Another interesting finding is that educational interventions were associated with significantly increased proximal adenoma detection rates. While the mechanisms for this change are not clearly explained by our results, several endoscopist-related factors could have been influenced by educational interventions, including technical skills, adequate air insufflation, washing and suctioning of debris and fluid, attention to flexures and folds, repetitive segment viewing, and torqueing maneuvers to enhance visualization. This finding is particularly important, given that missed proximal adenomas play an important role in the development of PCCRC 44 .
While our results are encouraging, one must interpret them with a degree of caution. When all studies (including RCTs using pre-intervention and post-intervention groups) were analyzed as having quasi-experimental designs, there were significant improvements in ADR. When the RCTs were considered separately using experimental and control groups, the improvement in ADR was less pronounced. This could lead one to hypothesize a potential contribution from the Hawthorne effect to our overall pooled results, whereby the behavior of study subjects has the ability to change merely from their knowledge of being surveilled 45 . Potential pitfalls of educational interventions also need close consideration. Expert facilitators and instructors are often required to deliver such interventions, and they are often not readily available. Furthermore, considerable preparation and considerable resources are required to successfully conduct such educational programs. The cost to the system associated with these interventions thus needs to be considered, even if one can ultimately make a strong argument for overall cost savings through quality improvement and reduction of disease burden. In addition, it is unknown whether there are differences in the degree of improvement when an endoscopist independently seeks out additional training, versus when it is mandated. Finally, the durability of any improvements in quality seen as a result of educational interventions is poorly established, given that the length of post-intervention follow-up was not uniformly reported across studies. Kaminski et al . included a long post-intervention phase of 18 months and found that ADR continued to be higher than the preintervention period, but less pronounced compared to the first 6 months post-intervention 29 . Conversely, the long-term sustainability of ADR improvement with the EQUIP-3 intervention is less clear 28 .
Of note, in a recent meta-analysis, we reported a significant association between endoscopist feedback and improvements in ADR, with a rate ratio of 1.21 38 . The rate ratio of 1.29 we report in our present study reflects a potential added impact of educational interventions. However, all but one study included in our analysis employed endoscopist audit and feedback concurrently with educational interventions. As endoscopist feedback has previously been independently associated with improved colonoscopy quality 38 , a potential confounding effect needs to be considered. The lone study assessing educational interventions alone (without feedback) in our analysis demonstrated non-statistically significant ADR improvements. Thus, further study is required to reliably determine the effect of educational interventions without any form of audit and feedback, and to assess the direct contributions of each of these measures on ADR and other quality indicators.
Our review has a number of strengths. A separate meta-analysis also recently evaluated the effect of educational interventions on ADR, but restricted inclusion to the 3 RCTs only, thereby missing several important studies assessing this question 46 . Furthermore, subgroup analyses were limited by the small number of input studies 46 . Our comprehensive search strategy included both randomized and non-randomized study designs as well as conference abstracts, thereby resulting in 13 studies included in our systematic review, with eight ultimately included in our quantitative meta-analysis. We also carried out several subgroup analyses to better understand potential sources of heterogeneity between studies. Importantly, we identified that studies restricted to primarily screening populations, the most common indication for colonoscopy, displayed considerably less inter-study heterogeneity. Lastly, we employed the GRADE approach to assess and summarize the certainty of the evidence leading to our conclusions.
Our study also has several limitations. For our overall analysis, we included only the interventional arms of RCTs and considered them as quasi-experimental studies in order to be able to compare them to the other included observational studies. However, to mitigate this, we also conducted a sensitivity analysis pooling only RCT data; the pooled interventional group still had ADR improvements compared to the control group. However, one should be cognizant that the degree of improvement seen with RCTs was somewhat lower than seen with quasi-experimental studies. This is in part owing to the fact that there was a (lesser) degree of ADR improvement in two of the RCT control groups as well. Thus, the overall pooled magnitude of ADR improvement should be interpreted with caution and in conjunction from the RCT-specific estimates. Secondly, there is a present lack of understanding of the mechanism(s) linking educational interventions with ADR improvement. This is important given that WT and CIR, whose improvements would be plausible mechanisms, remained unchanged. Thirdly, we opted to include gray literature. Although we believe this reduced publication bias, we acknowledge this may represent a limitation as it increases the heterogeneity due to incomplete details about the methodology and the lack of a peer review process. Encouragingly, in subgroup analyses, estimates of the primary outcome remained unchanged based on publication type. Finally, the majority of included studies were observational by design, and though attempts were made to report results adjusted for known confounders, the inability to adjust for unknown confounders must be acknowledged.
Conclusion
In conclusion, we found evidence that educational interventions improve ADR when conducted among independent endoscopists. Furthermore, they are also associated with improvements in pADR and overall PDR. Though the certainty of the evidence leading to conclusions on the primary outcome was low, we believe our findings are important. Future research should prioritize addressing important gaps, such as assessing the durability of the intervention, the impact on low- versus high-performers, and whether hands-on training or multimodal training are superior to didactic educational sessions.
Footnotes
Competing interests The authors declare that they have no conflict of interest.
Supplementary material :
References
- 1.American Cancer Society Key Statistics for Colorectal Cancer Atlanta, GA: American Cancer Society; 2020. Accessed: 2020 May 22https://www.cancer.org/cancer/colon-rectal-cancer/about/key-statistics.html
- 2.Vogelstein B, Fearon E R, Hamilton S R et al. Genetic alterations during colorectal-tumor development. N Engl J Med. 1988;319:525–532. doi: 10.1056/NEJM198809013190901. [DOI] [PubMed] [Google Scholar]
- 3.Zauber A G, Winawer S J, O'Brien M J et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med. 2012;366:687–696. doi: 10.1056/NEJMoa1100370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ran T, Cheng C Y, Misselwitz B et al. Cost-effectiveness of colorectal cancer screening strategies-a systematic review. Clin Gastroenterol Hepatol. 2019;17:1969–INF. doi: 10.1016/j.cgh.2019.01.014. [DOI] [PubMed] [Google Scholar]
- 5.Rex D K, Schoenfeld P S, Cohen J et al. Quality indicators for colonoscopy. Am J Gastroenterol. 2015;110:72–90. doi: 10.1038/ajg.2014.385. [DOI] [PubMed] [Google Scholar]
- 6.Rees C J, Gibson T S, Rutter M D et al. UK key performance indicators and quality assurance standards for colonoscopy. Gut. 2016;65:1923–1929. doi: 10.1136/gutjnl-2016-312044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kaminski M F, Regula J, Kraszewska E et al. Quality indicators for colonoscopy and the risk of interval cancer. N Engl J Med. 2010;362:1795–1803. doi: 10.1056/NEJMoa0907667. [DOI] [PubMed] [Google Scholar]
- 8.Singh S, Singh P P, Murad M H et al. Prevalence, risk factors, and outcomes of interval colorectal cancers: a systematic review and meta-analysis. Am J Gastroenterol. 2014;109:1375–1389. doi: 10.1038/ajg.2014.171. [DOI] [PubMed] [Google Scholar]
- 9.Morris E J, Rutter M D, Finan P J et al. Post-colonoscopy colorectal cancer (PCCRC) rates vary considerably depending on the method used to calculate them: a retrospective observational population-based study of PCCRC in the English National Health Service. Gut. 2015;64:1248–1256. doi: 10.1136/gutjnl-2014-308362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kaminski M F, Gibson T S, Bugajski M et al. Performance measures for lower gastrointestinal endoscopy: a European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative. Endoscopy. 2017;49:378–397. doi: 10.1055/s-0043-103411. [DOI] [PubMed] [Google Scholar]
- 11.Hilsden R J, Rose S M, Dube C et al. Defining and applying locally relevant benchmarks for the adenoma detection rate. Am J Gastroenterol. 2019;114:1315–1321. doi: 10.14309/ajg.0000000000000120. [DOI] [PubMed] [Google Scholar]
- 12.Mehrotra A, Morris M, Gourevitch R A et al. Physician characteristics associated with higher adenoma detection rate. Gastrointest Endosc. 2018;87:778–INF. doi: 10.1016/j.gie.2017.08.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ezaz G, Leffler D A, Beach S et al. Association between endoscopist personality and rate of adenoma detection. Clin Gastroenterol Hepatol. 2019;17:1571–INF. doi: 10.1016/j.cgh.2018.10.019. [DOI] [PubMed] [Google Scholar]
- 14.Sanaka M R, Gohel T, Podugu A et al. Adenoma and sessile serrated polyp detection rates: variation by patient sex and colonic segment but not specialty of the endoscopist. Dis Colon Rectum. 2014;57:1113–1119. doi: 10.1097/DCR.0000000000000183. [DOI] [PubMed] [Google Scholar]
- 15.Heresbach D, Barrioz T, Lapalus M G et al. Miss rate for colorectal neoplastic polyps: a prospective multicenter study of back-to-back video colonoscopies. Endoscopy. 2008;40:284–290. doi: 10.1055/s-2007-995618. [DOI] [PubMed] [Google Scholar]
- 16.Facciorusso A, Triantafyllou K, Murad M H et al. Compared Abilities of endoscopic techniques to increase colon adenoma detection rates: a network meta-analysis. Clin Gastroenterol Hepatol. 2019;17:2439–INF. doi: 10.1016/j.cgh.2018.11.058. [DOI] [PubMed] [Google Scholar]
- 17.Forbes N, Mohamed R, Raman M. Learning curve for endoscopy training: Is it all about numbers? Best Pract Res Clin Gastroenterol. 2016;30:349–356. doi: 10.1016/j.bpg.2016.04.003. [DOI] [PubMed] [Google Scholar]
- 18.Shaukat A, Oancea C, Bond J H et al. Variation in detection of adenomas and polyps by colonoscopy and change over time with a performance improvement program. Clin Gastroenterol Hepatol. 2009;7:1335–1340. doi: 10.1016/j.cgh.2009.07.027. [DOI] [PubMed] [Google Scholar]
- 19.Rajasekhar P T, Rees C J, Bramble M G et al. A multicenter pragmatic study of an evidence-based intervention to improve adenoma detection: the Quality Improvement in Colonoscopy (QIC) study. Endoscopy. 2015;47:217–224. doi: 10.1055/s-0034-1391563. [DOI] [PubMed] [Google Scholar]
- 20.Moher D, Shamseer L, Clarke M et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1. doi: 10.1186/2046-4053-4-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses Ottawa, ON: The Ottawa Hospital; 2019. Accessed: 2020 May 22http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
- 22.Guyatt G H, Oxman A D, Vist G E et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–926. doi: 10.1136/bmj.39489.470347.AD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Riley R D, Higgins J P, Deeks J J. Interpretation of random effects meta-analyses. BMJ. 2011;342:d549. doi: 10.1136/bmj.d549. [DOI] [PubMed] [Google Scholar]
- 24.Cochrane Handbook for Systematic Reviews of Interventions The Cochrane Collaboration; 2011. Accessed: 2020 May 22http://handbook-5-1.cochrane.org/front_page.htm
- 25.Egger M, Smith D G, Schneider M et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Begg C B, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–1101. [PubMed] [Google Scholar]
- 27.Coe S G, Crook J E, Diehl N N et al. An endoscopic quality improvement program improves detection of colorectal adenomas. Am J Gastroenterol. 2013;108:219–226. doi: 10.1038/ajg.2012.417. [DOI] [PubMed] [Google Scholar]
- 28.Wallace M B, Crook J E, Thomas C S et al. Effect of an endoscopic quality improvement program on adenoma detection rates: a multicenter cluster-randomized controlled trial in a clinical practice setting (EQUIP-3) Gastroint Endosc. 2017;85:538–545. doi: 10.1016/j.gie.2016.07.042. [DOI] [PubMed] [Google Scholar]
- 29.Kaminski M F, Anderson J, Valori R et al. Leadership training to improve adenoma detection rate in screening colonoscopy: A randomised trial. Gut. 2016;65:616–624. doi: 10.1136/gutjnl-2014-307503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Keswani R, Yadlapati R, Gleason K et al. Physician report cards and implementing standards of practice are both significantly associated with improved screening colonoscopy quality. Am J Gastroenterol. 2015;110:1134. doi: 10.1038/ajg.2015.103. [DOI] [PubMed] [Google Scholar]
- 31.Hall B, Benson M, Pfau P et al. Improved Adenoma detection rates at an academic gastroenterology unit following department colonoscopy assessment. Gastroint Endosc. 2010;71:AB107–108. [Google Scholar]
- 32.Corley D, Jensen C, Lee J et al. Increasing physician adenoma detection rate is associated with a reduced risk of post-colonoscopy colorectal cancer. Gastroenterology. 2019;156:S151. [Google Scholar]
- 33.Berger D, Hubbard E, Greenspan M et al. Non-neoplastic resection rate and adenoma detection rate increase after intervention to improve and monitor ADR. Gastroint Endosc. 2017;85:AB395. [Google Scholar]
- 34.Evans B, Pace D, Borgaonkar M et al. Effect of an educational intervention on colonoscopy quality outcomes. Surg Endosc. 2019 doi: 10.1007/s00464-019-07304-w. [DOI] [PubMed] [Google Scholar]
- 35.Rank J. Increased Adenoma Find Rate (AFR) and proportionately greater serrated adenoma find rate (safr) following a systematic quality improvement program in a large community gastroenterology practice. Gastroenterology. 2011;140:S199–200. [Google Scholar]
- 36.Salden B, Bouwens M, Winkens B et al. Systematic training improved the quality of colonoscopy by reducing the variation of quality indicators among providers. Gastroenterology. 2012;142:S2218. [Google Scholar]
- 37.Corley D A, Jensen C D, Marks A R et al. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med. 2014;370:1298–1306. doi: 10.1056/NEJMoa1309086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bishay K, Causada-Calo N, Scaffidi M A.Endoscopist feedback is associated with improvements in colonoscopy quality indicators: a systematic review and meta-analysis Gastroint Endosc 2020 10.1016/j.gie.2020.03.3865Online ahead of print. [DOI] [PubMed] [Google Scholar]
- 39.Madhoun M F, Tierney W M. The impact of video recording colonoscopy on adenoma detection rates. Gastroint Endosc. 2012;75:127–133. doi: 10.1016/j.gie.2011.07.048. [DOI] [PubMed] [Google Scholar]
- 40.Scaffidi M A, Grover S C, Carnahan H et al. A prospective comparison of live and video-based assessments of colonoscopy performance. Gastroint Endosc. 2018;87:766–775. doi: 10.1016/j.gie.2017.08.020. [DOI] [PubMed] [Google Scholar]
- 41.Waschke K A, Anderson J, Macintosh D et al. Training the gastrointestinal endoscopy trainer. Best Pract Res Clin Gastroenterol. 2016;30:409–419. doi: 10.1016/j.bpg.2016.05.001. [DOI] [PubMed] [Google Scholar]
- 42.Peyton J. Rickmansworth, UK: Manticore Europe Limited; 1998. Teaching and learning in medical practice. [Google Scholar]
- 43.Ekkelenkamp V E, Koch A D, de Man R A et al. Training and competence assessment in GI endoscopy: a systematic review. Gut. 2016;65:607–615. doi: 10.1136/gutjnl-2014-307173. [DOI] [PubMed] [Google Scholar]
- 44.le Clercq C M, Bouwens M W, Rondagh E J et al. Postcolonoscopy colorectal cancers are preventable: a population-based study. Gut. 2014;63:957–963. doi: 10.1136/gutjnl-2013-304880. [DOI] [PubMed] [Google Scholar]
- 45.Sedgwick P, Greenwood N. Understanding the Hawthorne effect. BMJ. 2015;351:h4672. doi: 10.1136/bmj.h4672. [DOI] [PubMed] [Google Scholar]
- 46.Lim S, Hammond S, Park J et al. Training interventions to improve adenoma detection rates during colonoscopy: a systematic review and meta-analysis. Surg Endosc. 2019 doi: 10.1007/s00464-019-07153-7. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.