
Figure 1.
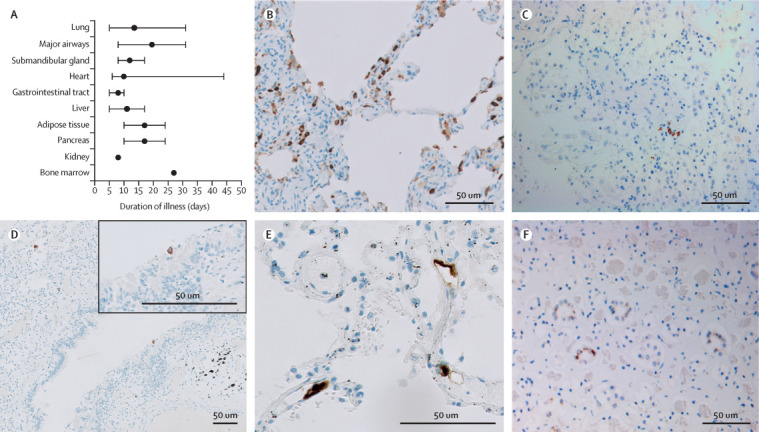
SARS-CoV-2 tropism
Two antibodies against SARS-CoV-2 nucleocapsid protein were used to detect infected cells. Staining of the same cell type by both antibodies was considered as positive immunoreactivity. (A) Median disease course per organ group with immunoreactivity for SARS-CoV-2. Error bars indicate the range. Adipose tissue consisted of mesocolic fat or omental fat (or both). The appendix (p 7)) shows SARS-CoV-2 positivity per organ per patient. (B) Stain against SARS-CoV-2 in the lung of a patient with mainly exudative diffuse alveolar damage and a disease course of 5 days. Immunoreactive cells were abundant (>10% infected cells per high-power field). Infected cells were pneumocytes along the alveolar walls, stromal cells in the septae, endothelial cells in the small blood vessels, and alveolar macrophages. (C) Stain against SARS-CoV-2 in the lung later in the disease course (patient with a disease course of 22 days) revealed only scattered immunoreactive cells, conceivably pneumocytes. (D) Stain against SARS-CoV-2 in the lung later in the disease course (patient with a disease course of 31 days) also showed immunopositivity in a respiratory cell lining a bronchiole. (E) Stain against SARS-CoV-2 in the lung early in the disease course (patient with a disease course of 5 days [also represented in part B]) showed immunopositive endothelial cells in septal capillaries. (F) Stain against SARS-CoV-2 in the kidney (patient with a disease course of 24 days) revealed immunoreactivity of the distal tubular epithelial cells. SARS-CoV-2=severe acute respiratory syndrome coronavirus 2.