
Figure 1.
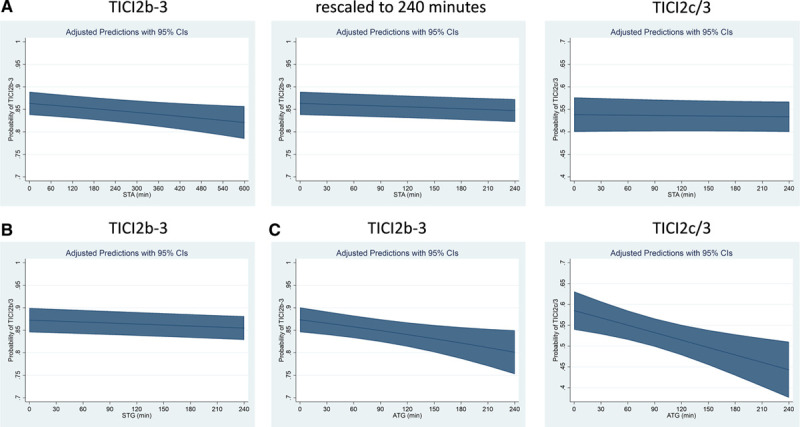
Association of symptom-onset-to-admission (STA) and admission-to-groin-puncture (ATG) intervals with the probability of achieving Thrombolysis in Cerebral Infarction (TICI) 2b-3 or 2c/3. Adjusted predicted probabilities of TICI 2b-3 or 2c/3 according to STA, symptom-onset-to-groin puncture (STG), and ATG intervals in minutes (see Methods). A, A small association of increasing STA with decreasing odds of achieving TICI 2b-3 was found (adjusted odds ratio [aOR], 0.96 [95%, 0.94–0.99] per hour) while no statistically significant association between STA and the odds of achieving TICI 2c/3 was observed (aOR, 0.99 [95% CI, 0.97–1.02] per hour). B, A small association of increasing STG with decreasing odds of achieving TICI 2b-3 was found (aOR, 0.96 [95%, 0.94–0.99] per hour). C, With increasing ATG, there was a strong reduction in the rates of TICI 2b-3 (aOR, 0.87 [95% CI, 0.79–0.96] per hour), corresponding to a 13% reduction in the odds of TICI 2b-3 per in-hospital hour delay. This association was also stable when considering TICI 2c/3 as relevant end point (aOR, 0.87 [95% CI, 0.79–0.95] per hour).