
Fig. 1.
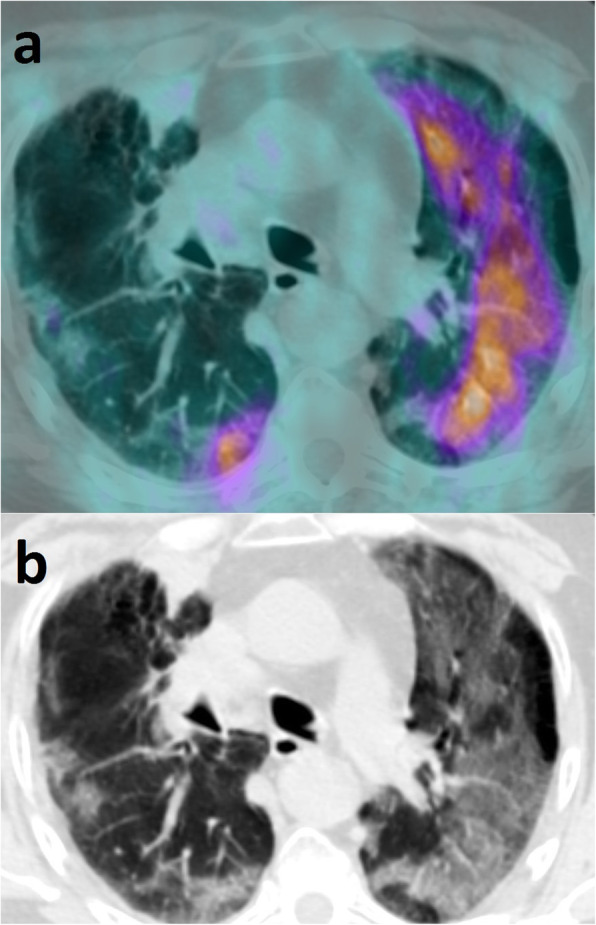
a Axial PET/CT view of the thorax showing diffuse, non-homogeneously increased FDG uptake (maximum SUV = 5) at the site of bilateral lung abnormalities. Additional images of pathologically increased FDG uptake were seen at the site of the primary tumor, in the apex of the right lung, and at the sites of multiple bone and liver metastases (not shown). No FDG-avid lymph-nodes were detected. b Corresponding CT view showing multifocal patchy centro-parenchymal and subpleural GGOs with subpleural fibrotic stripes of the right lung, as well as diffuse GGOs of the left lung with partial sparing of the subpleural space. Bronchial wall thickening and some bronchiectasis were also seen. No consolidations or micronodules, nor cysts or pleural effusion were detected. These features, in addition to the asymmetrical appearance and the sparing of the apical segments, orient, in first instance, towards an interstitial pneumonia of viral aetiology. In second instance, a pneumonitis induced by cisplatin-gemcitabine should be considered, as this is also characterized by multifocal or diffuse GGOs. Furthermore, although imaging features are not highly suspicious for Pneumocystis Jirovecii, the latter still represents a possible alternative diagnosis