

Abstract
Purpose:
To quantitatively assess anterior chamber and angle parameters by anterior segment optical coherence tomography (AS-OCT) in myopic eyes undergoing Implantable Collamer Lens (ICL V4c) implantation.
Methods:
Prospective noncomparative observational case series. Pre and postoperative (1st and 3rd month) AS-OCT angle parameters (anterior chamber depth [ACD], anterior chamber angle [ACA], Angle opening distance [AOD], trabecular iris space area [TISA], scleral spur angle [SSA]) were evaluated in 32 eyes (16 patients). SPSS version 20 with paired t-test for intragroup and Mann-Whitney U value test for intergroup comparisons.
Results:
It included 6 (37.5%) males and 10 (62.5%) females. Preoperative ACA of 34.6 ± 2.3° reduced to 32.2 ± 2.4°, 31.9 ± 2.5° at 1 and 3 months postoperatively (P = 0.001). Preoperative mean AOD500, AOD750, TISA500, TISA750, SSA of 0.34 ± 0.06 mm, 0.52 ± 0.15 mm, 0.09 ± 0.02 mm2, 0.20 ± 0.04 mm2, 34.27 ± 4.6° decreased to 0.32 ± 0.06 mm, 0.48 ± 0.15 mm, 0.08 ± 0.02 mm2, 0.17 ± 0.05 mm2, 32.5 ± 4.3° at 1-month (P = 0.001); 0.32 ± 0.06 mm, 0.47 ± 0.13 mm, 0.08 ± 0.02 mm2, 0.17 ± 0.05 mm2 and 32.4 ± 4.6° (P = 0.001) at 3-months, respectively. Correlation analysis between preoperative ACD/intraocular pressure (IOP) was − 0.62 (P = 0.0002) [1st month], −0.40 (0.024) [third month]; between IOP/postoperative ACA, AOD500, AOD750, TISA500, TISA750, SSA was − 0.04 (0.81), −0.03 (0.85), −0.08 (0.64), −0.12 (0.48), −0.10 (0.57), −0.06 (0.73) at 1 month; −0.09 (0.58), 0.04 (0.78), 0.12 (0.48), −0.02 (0.9), −0.04 (0.79), 0.02 (0.88) at 3 months; between ICL vault/ACA, AOD500, AOD750, TISA500, TISA750, SSA was 0.38 (0.02), 0.24 (0.17), 0.21 (0.25), 0.05 (0.75), 0.15 (0.41), 0.27 (0.13) at 1st month; 0.19 (0.28), 0.06 (0.71), −0.03 (0.85), 0.005 (0.97), 0.05 (0.78), 0.07 (0.68) at 3rd month.
Conclusion:
Postoperatively significant angle narrowing was noted. There was a negative correlation between IOP and preoperative ACD. There was no significant correlation between IOP and ICL vault with postoperative AS-OCT angle parameters.
Keywords: Angle, anterior chamber, anterior segment optical coherence tomography, ICL V4c, myopia, phakic IOL
The use of Visian Implantable Collamer Lenses (ICLs, STAAR Surgical, Monrovia, CA, USA), which are soft, foldable, sulcus-placed posterior chamber phakic intraocular lenses, is a well-accepted surgical treatment for high myopic refractive errors.[1,2,3] ICL implantation for high-myopic correction has resulted in significant changes in anterior chamber angle (ACA), depth and volume.[4] The iridocorneal angle was noted to have narrowing in different quadrants after ICL-V4c implantation, which remained stable at 3 months in photopic and scotopic conditions.[5,6] In view of the increasing adoption of ICL, this study of the AC parameters measurements in ICL was undertaken.[7,8]
Methods
Study design
This was a prospective, longitudinal, noncomparative observational, pilot study that was done in accordance with the tenets of the Declaration of Helsinki. Ethical clearance was obtained. Thirty-two eyes of 16 patients with high myopia undergoing ICL V4c implantation, between the age of 20 and 40 years with a stable refractive error for the previous 2 years who were not amenable to laser refractive surgery correction and willing to participate in the study were included. All patients with pathological myopia, anterior chamber depth (ACD) less than 2.8 mm, previous history of ocular inflammation or glaucoma, and concurrent corneal or retinal disease and specular count less than 2500 cells/mm2 were excluded from the study. All surgeries were performed by a single surgeon by following a standard protocol.
Data collection
The preoperative details included uncorrected visual acuity (UCVA), best-corrected visual acuity (BCVA), refractive error, slit-lamp examination, intraocular pressure (IOP), pachymetry, endothelial cell count, anterior segment optical coherence tomography (AS-OCT) imaging (Visante, Carl Zeiss Meditec AG, Germany) for iridocorneal angle dimensions. Postoperative UCVA, BCVA, IOP, lens vault (distance between ICL and the anterior surface of lens), ACD, AS-OCT iridocorneal angle measurements were performed at 1 and 3 months. Angle parameters and ICL vault were obtained from AS-OCT images captured by an expert technician [Fig. 1]. The trabecular iris angle (TIA) was measured by tracing a line of 500 μm from the angle recess towards the Schwalbe line and another line on the surface of the iris to the point perpendicular to the first line. The ICL vault was measured by tracing a line from the center of the anterior pole of the crystalline lens to the posterior pole of the ICL. Three scans were taken, and the best quality image was chosen. Angle opening distance 500 μm from the scleral spur (AOD 500; perpendicular distance from the trabecular meshwork 500 μm anteriorly from the scleral spur to the anterior iris surface), Trabecular iris space area 500 μm (TISA500; area bounded anteriorly by AOD, posteriorly by a line from the scleral spur perpendicular to the line of the inner scleral wall to the opposing iris, superiorly by the corneoscleral wall and inferiorly by the iris surface). Similarly, AOD and TISA were measured at 750 μm.[9,10] Scleral spur angle (SSA) was also measured using AS-OCT.
Figure 1.
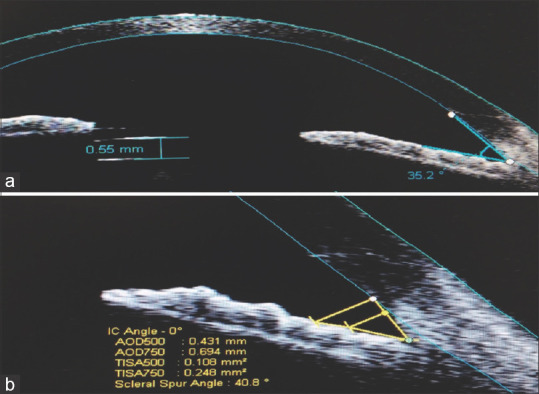
Postoperative anterior segment optical coherence tomography (AS-OCT) picture depicting ACD and Implantable Collamer Lens (ICL) vault (a) and anterior chamber angle parameters measurement (AOD500, AOD750, TISA500, TISA750, ACA and SSA) (b) AOD500: angle opening distance at 500μ; AOD750: angle opening distance at 750μ; TISA500: trabecular iris space area at 500 μ; TISA750: trabecular iris space area at 750μ; ACA: anterior chamber angle; SSA: scleral spur angle
Surgical technique
All surgeries were done under topical anesthesia using 0.5% proparacaine hydrochloride. Pupillary dilatation was achieved with a combination of eye drops containing 1% tropicamide and 2.5% phenylephrine. With a temporal approach, two 1 mm paracentesis ports were made using angled keratome or 15° micro-vitreoretinal blade at 12 and 6 o'clock positions. Hypromellose 2% (Viscomet PF, Unimed technologies) viscoelastic was then injected into the AC by taking care not to overfill the chamber. A temporal 3.2 mm clear corneal incision was made using keratome. The ICL was loaded into the cartridge and injected into the AC. The two paracentesis incisions were used to position the footplates under the iris using the special manipulating instrument (Vukich's manipulator) to ensure that all haptics were tucked posterior to the iris. In the case of toric ICL (TICL) proper alignment was ensured. At the end of the surgery, viscoelastic was cleared from the AC. A standard postoperative regime consisting of topical prednisolone acetate 1% four times a day for 5 days tapering over 2 weeks and topical moxifloxacin 0.5% four times a day for 2 weeks was followed. Postoperatively, the patient was examined at day 1 to check for proper ICL positioning and lens vault on slit-lamp and AS-OCT, and IOP was checked. The patient was followed up regularly at 1 week, 1 month, 3 months, and 6 months after the surgery. UCVA, BCVA, IOP, central corneal thickness (CCT), ICL vault, and ACD, angle parameters (ACA, AOD500, AOD750, TISA500, TISA750, SSA) were measured using AS-OCT at 1 month and 3 months postoperative period.
Outcome measures
The primary outcome measure was to assess the changes in IOP, ACD, ACA, AOD 500 and 750, TISA 500 and 750, and SSA after ICL V4c implantation at postoperative day 1, month 1 and 3, and secondary outcome measure was to assess correlation of IOP and ICL lens vault, with the AS-OCT ACA parameter measurements.
Statistical analysis
The data was analyzed using SPSS version 20 (Statistical Package for Social Sciences) with paired t-test for intragroup comparison and Mann-Whitney U value test for intergroup comparison. P value of less than 0.05 was considered significant.
Results
Thirty-two eyes of 16 patients were included in this study, of which 10 (62.5%) were females and 6 (37.5%) were males. The mean age of presentation was 28.7 ± 3.2 years. The mean size of the ICL V4c implanted was 13.2 ± 0.34 mm with a mean spherical power of − 10.43 ± 3.12 diopters and mean cylindrical power of 2.21 ± 0.21 dioptres. The mean preoperative ACD was 3.25 ± 0.15 mm (2.95–3.5 mm). The study characteristics are depicted in Table 1; Figs. 2 and 3.
Table 1.
Details of the study characteristics, their comparison in the preoperative and postoperative period
| Study parameters | Preoperative | Postoperative | |
|---|---|---|---|
| 1 month | 3 months | ||
| Mean intraocular pressure (IOP) (mmHg) | 13.8±1.39 | 15.37±2.58 *P=0.021 |
14.93±1.77 *P=0.05 |
| Mean ICL vault (μm) | - | 600±60 | 580±50 |
| (**P=0.02) | |||
| Trabecular iris angle (TIA) (degrees) | 34.684±2.34 | 32.2±2.4 (*P=001) |
31.9±2.5 (*P=001) |
| Mean angle opening distance 500 (AOD500) (mm) | 0.349±0.61 | 0.32±0.06 (*P=0.001) |
0.32±0.06 (*P=0.001) |
| Mean AOD 750 (mm) | 0.521±0.16 | 0.48±0.15 (*P=0.001) |
0.47±0.13 (*P=0.001) |
| Mean trabecular iris space area 500 (TISA 500) (mm2) | 0.098±0.02 | 0.08±0.02 (*P=0.001) |
0.08±0.02 (*P=0.001) |
| Mean TISA 750 (mm2) | 0.202±0.04 | 0.17±0.05 (*P=0.001) |
0.17±0.05 (*P=0.001) |
| Mean scleral spur angle (SSA) (degrees) | 34.278±4.62 | 32.5±4.3 (*P=0.001) |
32.4±4.6 (*P=0.001) |
*Paired t-test (in comparison to preoperative value). **Paired t-test (between postoperative months 1 and 3 value) ICL: Implantable Collamer Lens
Figure 2.

(a) Box whiskers plot showing the intraocular pressure at baseline, 1st month and 3rd-month postoperative period. (b) Box whiskers plot showing the ICL vault at 1st month and 3rd-month postoperative period
Figure 3.

Correlation between intraocular pressure (IOP) and angle parameters at postoperative 1 month (I) and the correlation between IOP and angle parameters at postoperative 3rd month (II)
The mean preoperative ACA was 34.68 ± 2.34° which decreased to 32.201 ± 2.453 at 1 month (P = 0.001) and 31.94 ± 2.52 at 3 months post-op period (P < 0.001). The mean preoperative values of AOD 500 and AOD 750 were 0.35 ± 0.06 mm and 0.52 ± 0.15 mm respectively both of which decreased at 1 month postoperative period to 0.324 ± 0.059 (0.001) and 0.482 ± 0.151 (0.001) and at 3 months postoperative period to 0.32 ± 0.06 (0.001) and 0.47 ± 0.13 (0.001), respectively (P < 0.001). The mean preoperative values of TISA 500 and TISA 750 were 0.09 ± 0.02 mm2 and 0.2 ± 0.04 mm2, respectively both of which decreased at one month postoperative period to 0.08 ± 0.02 (0.001) and 0.17 ± 0.05 (P = 0.001) and 3 months post-op period to 0.08 ± 0.02 and 0.17 ± 0.05 (P < 0.001), respectively. The mean value of SSA was 34.28 ± 4.6° preoperatively which decreased to 32.5 ± 4.3° (P = 0.001) and to 32.4 ± 4.6° at 1 month and 3 months postoperative period, respectively (P < 0.001). It is to be noted that there was no significant difference in any of these parameters between 1 month and 3 months postoperative period.
Preoperative IOP of 13.8 ± 1.39 increased to 15.37 ± 2.58 (P = 0.021) and to 14.93 ± 1.77 at 3rd month (P = 0.05). There was no significant difference between IOP at 1st month and 3rd month (P = 0.61). Vault at 1 month was 0.60 ± 0.06 and decreases significantly at 3rd month to 0.58 ± 0.05 (P = 0.02). There was a significant negative correlation between the preoperative ACD and the IOP at postoperative 1st and 3rd month. The Pearson correlation coefficient between preoperative ACD and the IOP at 1st and 3rd month was noted to be − 0.6185 (P = 0.0002) and − 0.3976 (0.0242), respectively.
Analysis for correlation of IOP and ICL vault with AC parameters at postoperative months 1 and 3 [Table 2; Figs. 3 and 4] did not reveal any significant correlation. None of the patients needed exchange or explantation of the ICL V4c in our study. No other complications such as postoperative uveitis, angle-closure attacks, cataract formation, retinal detachment, or endophthalmitis were noted in this study.
Table 2.
Correlation analysis of postoperative IOP and ICL vault with anterior chamber angle parameters
| Study variable | ACA | AOD500 | AOD750 | TISA500 | TISA750 | SSA |
|---|---|---|---|---|---|---|
| Postoperative month 1 r (P) | ||||||
| IOP | −0.04 (0.81) | −0.033 (0.85) | −0.083 (0.64) | −0.12 (0.48) | −0.10 (0.57) | −0.06 (0.73) |
| VAULT | 0.38 (0.02) | 0.24 (0.17) | 0.21 (0.25) | 0.05 (0.75) | 0.15 (0.41) | 0.27 (0.13) |
| Postoperative month 3 r (P) | ||||||
| IOP | −0.09 (0.58) | 0.04 (0.78) | 0.12 (0.48) | −0.02 (0.9) | −0.04 (0.79) | 0.02 (0.88) |
| VAULT | 0.19 (0.28) | 0.06 (0.71) | −0.03 (0.85) | 0.005 (0.97) | 0.05 (0.78) | 0.07 (0.68) |
r (P): Pearson’s correlation coefficient, P value; ACA: Anterior chamber angle; AOD500: Angle opening distance at 500μ; AOD750: Angle opening distance at 750μ; TISA500: Trabecular iris space area at 500μ; TISA750: Trabecular iris space area at 750μ; SSA: Scleral spur angle
Figure 4.

Correlation between ICL vault and angle parameters at postoperative 1 month (i) and the correlation between ICL vault and angle parameters at postoperative 3rd month (II)
Discussion
ICL is an FDA-approved modality for refractive correction in patient unsuitable for corneal ablation. It is reversible procedure and can correct wide range of refractive errors including myopia, hypermetropia, and astigmatism.[11] The most recently introduced model of ICL is V4c, which has central small opening known as CentraFLOW. It comes with various advantages including no need of peripheral iridotomy (PI) preoperatively, decreased risk of pigment dispersion, intraoperative thorough viscoelastic removal, decreased risk of pupillary block glaucoma, decreasing cataract formation as continuous aqueous current between anterior capsule of lens and posterior surface of ICL is maintained.[12] Preoperative ICL planning includes two important parameters that help in choosing appropriate size of lens in particular patient, assessment of ACD, and white-to-white measurement. The ICL sizing has been described in Table 3.
Table 3.
Pre-operative assessment of ICL sizing based on white to white (WTW) and anterior chamber depth (ACD)
| White to white (mm) | ACD (mm) | ICL size |
|---|---|---|
| <10.5 | All | Not recommended |
| 10.5-10.6 | <=3.5 | Not recommended |
| 10.5-10.6 | >3.5 | 12.1 |
| 10.7-11.0 | All | 12.1 |
| 11.1 | <=3.5 | 12.1 |
| 11.1 | >3.5 | 12.6 |
| 11.2-11.4 | All | 12.6 |
| 11.5-11.6 | <=3.5 | 12.6 |
| 11.5-11.6 | >3.5 | 13.2 |
| 11.7-12.1 | All | 13.2 |
| 12.2 | <=3.5 | 13.2 |
| 12.2 | >3.5 | 13.7 |
| 12.3-12.9 | All | 13.7 |
| >=13 | All | Not recommended |
Higueras-Esteban et al. compared the V4B and V4C design of ICL to evaluate the safety of V4C ICL without iridotomy.[13] They did not find any significant difference between the two designs in terms of IOP and vault in the postoperative period. So, they reached a conclusion that the new ICL with the CentraFLOW provides similar results as its predecessors for correcting moderate to high myopia and maintaining safe IOP levels without the need of iridotomy. Our study also corroborates the above findings. Even though an increase in IOP is seen in the postoperative period, it remains in the physiologic range and there is no record of any acute/very high increase in IOP in any of our case. Shimizu et al. long-term comparison of conventional ICL and ICL with hole evaluated the safety, efficacy, predictability, change in IOP and ACD in the postoperative period and compared the two designs of ICL.[14] They did not find any significant change in the IOP in the Hole ICL group or in the conventional ICL group. No significant increase in IOP (>21 mmHg) was noted during the 5-year observation period. Hole ICL group was associated with a significant change in the ACD but not the conventional ICL group. Multiple comparisons demonstrated significant difference between preoperative and postoperative measurements of ACD. We also saw similar findings with the IOP remaining in the normal range in all the cases. Also, the angle parameters as measured by AS-OCT showed a significant decrease as is seen in the above study in terms of ACD.
Eissa et al. have done a study to evaluate ACA after ICL implantation.[15] They enrolled 54 eyes of 27 patients undergoing V4C phakic posterior chamber Collamer lens implantation for myopic refractive correction. They found a significant increase in IOP which remained the same at 6 and 18 months. ACA measured using Pentacam imaging was found to decrease significantly at 1, 6, and 18 months. They noted a moderate correlation between ICL vault and AC angle. They had concluded that ICL implantation leads to an increase in IOP and a decrease in the AC angle with all values maintaining in the physiological range. This study of 32 eyes of 16 patients evaluated the ACA using AS-OCT. We found similar results with the IOP increasing at 1st month and remaining the same in the 3rd-month postoperative period. The ACA parameters as measured by AS-OCT showed a significant decrease at 1 and 3 months postoperative period. As against the above study, we did not find any significant correlation between IOP, ICL vault, and ACA parameters, but found a significant negative correlation between the preoperative ACD and the postoperative IOP.
Zhu et al. evaluated the AC volume (ACV) (Pentacam imaging) after ICL implantation in 45 eyes of 26 patients with high myopia preoperatively and postoperatively over a mean follow-up period of 4.28 months.[16] The mean ACV was found to decrease significantly (a decrease of 40%) from 198.33 ± 33.08 mm3 before surgery to 118.65 ± 17.70 mm3 after surgery. They found a positive correlation between postoperative ACV and ACA and concluded the ACV to be a sensitive parameter that is complementary to vault and ACD in preoperative assessment and postoperative monitoring of ICL patients.
We used AS-OCT imaging to assess the ACA parameters. This study shows similar results with the angle parameters decreasing significantly in the postoperative period. Postoperative IOP shows a negative correlation with the preoperative ACD. The above two findings enhance the importance of measuring ACD as well as angle parameters which can act as a guide while selecting ideal candidates for ICL surgery.
Elmohamady et al. evaluated AC changes after ICL implantation in 34 patients with high myopia who underwent ICL implantation using Pentacam imaging and noted that the average ACA decreased significantly from 36.93° ± 4.75° preoperatively to 25.17° ± 5.64° and 25.23° ± 6.05° at 1 and 3 months, postoperatively.[17] Mean ACV was 191.24 ± 11.18 mm3 preoperatively which reduced significantly to 141.53 ± 16.77 and 142.11 ± 15.89 mm3 at 1 and 3 months, postoperatively. Mean central AC depth was 3.59 ± 0.17 mm preoperatively and decreased to 2.83 ± 0.24 mm and 2.96 ± 0.25 mm at 1 and 3 months postoperatively. The ICL vault decreased significantly (P- value <0.001) from 0.556 ± 0.033 mm at 1 month postoperative period to 0.431 ± 0.056 mm at 3 months postoperatively. They concluded that ICL implantation leads to a significant decrease in ACA, volume, and depth. Our results also concur with their findings with the angle parameters in our study decreasing significantly in the postoperative period as well as vault decreasing from postoperative 1st month to 3rd month.
Yan et al. have reported the 2-year outcomes of Visian ICLwith a central hole (ICL V4c) implantation for correcting high myopia in 61 eyes of 32 patients using Scheimpflug tomography imaging to measure ACV, ACD, ACA width (ACAW), and vault.[18] The ACV, ACD, and ACAW were noted to reduce from preoperative values of 193.28 ± 29.15 mm3, 3.15 ± 0.23 mm, and 36.51 ± 6.54° to 112.48 ± 17.01 mm3, 2.99 ± 0.23 mm, and 22.54 ± 5.27° (P = 0.0008, 0.008, and 0.0003, respectively). IOP did not show any increase in comparing preoperative and postoperative values. It was seen to be 15.39 ± 2.88 mmHg before surgery and 15.86 ± 4.11 mmHg at 2 years (P = 0.11).
This study shows a significant narrowing of the ACA parameters at postoperative months 1 and 3, in comparison to the preoperative values. We noted that all the AS-OCT ACA parameters TIA, AOD 500, AOD 750, TISA 500, TISA 750, and SSA reduced significantly (P = 0.001) at 1 month and 3 months (P = 0.001) postoperatively when compared to the preoperative values. No significant difference was noted between 1 month and 3 months postoperative values (P = 0.21). Preoperative IOP of 13.8 ± 1.39 mmHg increased to 15.37 ± 2.58 mmHg (P = 0.021) and to 14.93 ± 1.77 mmHg at 3rd month (P = 0.05). There was no significant difference between IOP at 1st month and 3rd month (P-value = 0.61). Though considerable angle narrowing was detected at both 1 and 3 months after ICL V4c implantation, there seemed no correlation between the IOP, ICL vault, and the ACA parameters which is suggestive that the CentraFLOW design precludes the affection on the IOP despite ACA narrowing caused by the ICL implantation in the sulcus. There was a significant negative correlation between the preoperative ACD and the IOP at 1st month and 3rd month postoperatively [r = −0.6185 (P = 0.0002) and r = −0.3976 (0.024), respectively]. Considering that the ACA parameters narrow significantly in the postoperative period, preoperative AS-OCT measurement of angle parameters may be useful in identifying candidates suitable for ICL implantation. Those candidates with preoperative narrow-angle chamber parameters may be excluded from ICL implantation even with the V4c model with the CentraFLOW design.
Conclusion
ICLV4C is a safe approach to correcting myopia without the need for iridotomy, thus, avoiding the associated inflammation. An increase in IOP is seen in the postoperative period which remains in the physiologic range. The negative correlation between the preoperative ACD and postoperative IOP as well as the significant decrease seen in the AS-OCT angle parameters, both reinforce the importance of measuring the angle parameters before taking up the patient for an ICL surgery.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Sanders DR, Doney K, Poco M. United States Food and Drug Administration clinical trial of the Implantable Collamer Lens (ICL) for moderate to high myopia: Three-year follow-up. Ophthalmology. 2004;111:1683–92. doi: 10.1016/j.ophtha.2004.03.026. [DOI] [PubMed] [Google Scholar]
- 2.Sanders DR, Schneider D, Martin R, Brown D, Dulaney D, Vukich J, et al. Toric Implantable Collamer Lens for moderate to high myopic astigmatism. Ophthalmology. 2007;114:54–61. doi: 10.1016/j.ophtha.2006.08.049. [DOI] [PubMed] [Google Scholar]
- 3.Lovisolo CF, Reinstein DZ. Phakic intraocular lenses. Surv Ophthalmol. 2005;50:549–87. doi: 10.1016/j.survophthal.2005.08.011. [DOI] [PubMed] [Google Scholar]
- 4.Elmohamady MN, Abdelghaffar W. Anterior chamber changes after Implantable Collamer Lens implantation in high myopia using pentacam: A prospective study. Ophthalmol Ther. 2017;6:343–9. doi: 10.1007/s40123-017-0109-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fernández-Vigo JI, Macarro-Merino A, Fernández-Vigo C, Fernández-Vigo JÁ, Martínez-de-la-Casa JM, Fernández-Pérez C, et al. Effects of Implantable Collamer Lens V4c placement on iridocorneal angle measurements by Fourier-domain optical coherence tomography. Am J Ophthalmol. 2016;162:43–52e1. doi: 10.1016/j.ajo.2015.11.010. [DOI] [PubMed] [Google Scholar]
- 6.Garcia-De la Rosa G, Olivo-Payne A, Serna-Ojeda JC, Salazar-Ramos MS, Lichtinger A, Gomez-Bastar A, et al. Anterior segment optical coherence tomography angle and vault analysis after toric and non-toric Implantable Collamer Lens V4c implantation in patients with high myopia. Br J Ophthalmol. 2018;102:544–8. doi: 10.1136/bjophthalmol-2017-310518. [DOI] [PubMed] [Google Scholar]
- 7.Kamiya K, Shimizu K, Igarashi A, Kitazawa Y, Kojima T, Nakamura T, et al. Posterior chamber phakic intraocular lens implantation: Comparative, multicentre study in 351 eyes with low-to-moderate or high myopia. Br J Ophthalmol. 2018;102:177–81. doi: 10.1136/bjophthalmol-2017-310164. [DOI] [PubMed] [Google Scholar]
- 8.Dougherty PJ, Priver T. Refractive outcomes and safety of the Implantable Collamer Lens in young low-to-moderate myopes. Clin Ophthalmol Auckl NZ. 2017;11:273–77. doi: 10.2147/OPTH.S120427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chen X, Miao H, Naidu RK, Wang X, Zhou X. Comparison of early changes in and factors affecting vault following posterior chamber phakic Implantable Collamer Lens implantation without and with a central hole (ICL V4 and ICL V4c) BMC Ophthalmol. 2016;16:161. doi: 10.1186/s12886-016-0336-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Fernández-Vigo JI1, García-Feijóo J, Martínez-de-la-Casa JM, García-Bella J, Fernández-Vigo JA. Morphometry of the trabecular meshwork in vivo in a healthy population using Fourier-domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2015;56:1782–8. doi: 10.1167/iovs.14-16154. [DOI] [PubMed] [Google Scholar]
- 11.Kamiya K, Shimizu K, Igarashi A, Hikita F, Komatsu M. Four-year follow-up of posterior chamber phakic intraocular lens implantation for moderate to high myopia. Arch Ophthalmol. 2009;127:845–50. doi: 10.1001/archophthalmol.2009.67. [DOI] [PubMed] [Google Scholar]
- 12.Packer M. The Implantable Collamer Lens with a central port: Review of the literature. Clin Ophthalmol. 2018;12:2427–38. doi: 10.2147/OPTH.S188785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Higueras-Esteban A, Ortiz-Gomariz A, Gutiérrez-Ortega R, Villa-Collar C, Abad-Montes JP, Fernandes P, et al. Intraocular pressure after implantation of the Visian Implantable Collamer Lens with CentraFLOW without iridotomy. Am J Ophthalmol. 2013;156:800–5. doi: 10.1016/j.ajo.2013.05.018. [DOI] [PubMed] [Google Scholar]
- 14.Shimizu K, Kamiya K, Igarashi A, Kobashi H. Long-term comparison of posterior chamber phakic intraocular lens with and without a central hole (Hole ICL and conventional ICL) implantation for moderate to high myopia and myopic astigmatism. Medicine (Baltimore) 2016;95:e3270. doi: 10.1097/MD.0000000000003270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Eissa SA, Sadek SH, El-Deeb MWA. Anterior chamber angle evaluation following phakic posterior chamber Collamer lens with CentraFLOW and its correlation with ICL vault and intraocular pressure. J Ophthalmol. 2016;2016:1383–89. doi: 10.1155/2016/1383289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zhu Y, Zhu H, Jia Y, Zhou J. Changes in anterior chamber volume after implantation of posterior chamber phakic intraocular lens in high myopia. BMC Ophthalmol. 2018;18:185. doi: 10.1186/s12886-018-0830-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Elmohamady MN, Abdelghaffar W. Anterior chamber changes after Implantable Collamer Lens implantation in high myopia using Pentacam: A prospective study. Ophthalmol Ther. 2017;6:343–9. doi: 10.1007/s40123-017-0109-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yan Z, Miao H, Zhao F, Wang X, Chen X, Li M, et al. Two-year outcomes of Visian Implantable Collamer Lens with a central hole for correcting high myopia? J Ophthalmol. 2018;2018:8678352. doi: 10.1155/2018/8678352. doi: 10.1155/2018/8678352. [DOI] [PMC free article] [PubMed] [Google Scholar]