

Purpose of review
To review the recent literature on the burden of eating disorders in terms of mortality, disability, quality of life, economic cost, and family burden, compared with people without an eating disorder.
Recent findings
Estimates are that yearly over 3.3 million healthy life years worldwide are lost because of eating disorders. In contrast to other mental disorders, in anorexia nervosa and bulimia nervosa years lived with disability (YLDs) have increased. Despite treatment advances, mortality rates of anorexia nervosa and bulimia nervosa remain very high: those who have received inpatient treatment for anorexia nervosa still have a more than five times increased mortality risk. Mortality risks for bulimia nervosa, and for anorexia nervosa treated outside the hospital, are lower but still about twice those of controls. In people with an eating disorder, quality of life is reduced, yearly healthcare costs are 48% higher than in the general population, the presence of mental health comorbidity is associated with 48% lower yearly earnings, the number of offspring is reduced, and risks for adverse pregnancy and neonatal outcomes are increased.
Summary
People with a current or former eating disorder are at risk of increased mortality, high YLD rates, a reduced quality of life, increased costs, and problems with childbearing.
Keywords: eating disorders, economic cost, mortality, quality of life, years lived with disability
INTRODUCTION
’Eating disorders are disabling, deadly, and costly mental disorders that considerably impair physical health and disrupt psychosocial functioning’, as Treasure et al. [1] state. This makes effective treatments the more important. For bulimia nervosa [2,3] and binge eating disorder (BED) [4], there are effective psychological treatments, especially cognitive behaviour therapy (CBT). However, for anorexia nervosa, a recent meta-analysis could not establish its efficacy over an active control condition [5]. For the most severe and enduring cases of anorexia nervosa, there is a paucity of evidence-based treatments [6].
The efficacy of treatment (or lack thereof) is reflected in illness duration and remission rates. A series of publications on very long-term (10–20 years) follow-up studies of inpatients with an eating disorder showed that, respectively 64% of persons previously diagnosed with anorexia nervosa, 53% of those previously diagnosed with bulimia nervosa, and 30% of those previously diagnosed with BED, still met diagnostic criteria for an eating disorder at follow-up; a further 6% for anorexia nervosa, 9% for bulimia nervosa and 31% for BED had remaining eating disorder symptoms [7,8▪▪,9]. Higher recovery rates of anorexia nervosa were reported in two smaller long-term (≥20 years) follow-up studies of adolescent-onset anorexia nervosa; one on an outpatient sample [10], the other on a community sample [11▪▪]. In both studies, around 65% of the cases were in complete remission at follow-up. Thus, across eating disorders, a considerable 62–70% of people who had received inpatient treatment and 35% who had received outpatient treatment, still met full diagnostic criteria or had remaining eating disorder symptoms at long-term follow-up.
Protracted eating disorder pathology means that eating disorders have a great impact on the present and future health and quality of life of affected persons, their caregivers and society. In this journal in 2016, Erskine et al.[12] described the inclusion of eating disorders in the Global Burden of Disease (GBD) study in 2010 as a watershed in the recognition of these disorders in the wider global health community, and presented findings on the burden of eating disorders from the GBD 2013 database. Here we review current GBD data on eating disorders. Furthermore, we widen the scope of burden to address some of the limitations of the GBD concept of burden as ‘within-the-skin’ health loss: as Erskine et al.[12] noted, the impact of eating disorders on families and other support systems is neither reflected in the GBD burden estimates nor do they represent the future adverse impact of an eating disorder on an individual's psychological and economic well being. And as only anorexia nervosa and bulimia nervosa have so far been included for burden quantification, the GBD data only pertain to a subset of eating disorders. This review addresses eating disorder-related mortality, disability, economic cost, and other individual, caregiver and family burden.
Box 1.
no caption available
METHODS
This review is based on a literature search using Medline and Pre-Medline, Medline Epub ahead of print and in-process and other nonindexed citations, and Embase psychiatry resources (via OvidSP), using several key terms relating to eating disorders and burden (terms on request available from the first author). We supplemented the results with Google Scholar searches for specific combinations of terms. The search was conducted up to 8 May 2020. We limited the search to publications in English from 2018 onwards and to studies reporting on formal eating disorder diagnoses [anorexia nervosa, bulimia nervosa, BED, Avoidant/Restrictive Food Intake Disorder (ARFID)]. The titles and abstracts of 1234 unique listings were screened by the first author for relevance. Studies in which eating disorders were comorbid with other health conditions (e.g. diabetes) were excluded, as well as studies on fewer than 25 subjects. In order to put information in perspective, we focussed on studies that used population-based metrics or that compared people with an eating disorder to noneating disorder controls.
GLOBAL BURDEN OF DISEASE STUDY
A major global effort to gather, combine, and compare information on the burden associated with a large range of disorders, both somatic and mental, is the ongoing Global Burden of Disease (GBD) study, which started in 1990. Information is regularly updated and available online through the Global Health Data Exchange (GHDx) site of the Institute of Health Metrics and Evaluation (Seattle, Washington, USA): http://ghdx.healthdata.org/. Anorexia nervosa and bulimia nervosa have been included since the GBD 2010 study.
The burden of disease is defined as the gap between current health status and an ideal situation in which everyone lives into old age free of disease and disability. Causes of the gap are premature mortality, disability, and exposure to certain risk factors that contribute to illness. An important metric to express this gap is the disability-adjusted life year (DALY). One DALY expresses one lost year of ‘healthy’ life. The burden of a disease is the sum of DALYs for this specific disease across a population. DALYs are calculated as the sum of the years of life lost (YLL) because of premature mortality and the years lost due to disability (YLD), thus incorporating both mortality and morbidity information. Using DALYs, the burdens of various diseases can be compared, from those that cause premature death but little disability to those that cause disability but not death.
For mental health disorders, YLD are the main contributors towards DALYs. Table 1 shows the GBD 2017 data on YLD for eating disorders, all mental disorders (substance use disorders not included), all noncommunicable diseases (of which mental disorders are part), and all causes [13▪,14].
Table 1.
Global Burden of Disease 2017: counts, age-standardized rates per 100 000 population, and percentage change from 2007 to 2017 for years lived with disability (YLD)
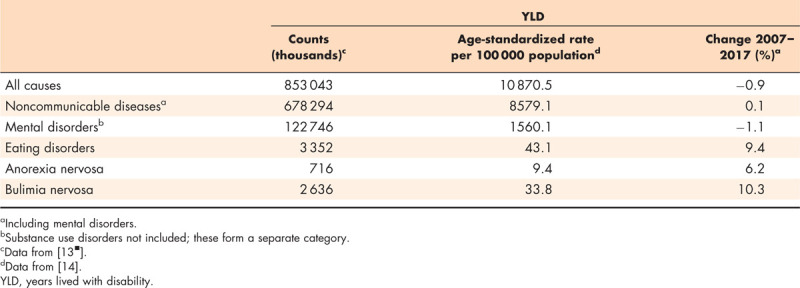
It was estimated that in 2017, worldwide over 3.3 million healthy life years were lost to eating disorder-related disability, amounting to an age-standardized YLD rate of 9.4 for anorexia nervosa, and 33.8 for bulimia nervosa, per 100 000 population. YLD rates for eating disorders contributed 2.8% to the overall YLD load of mental disorders. Whereas from 2007 to 2017, YLD rates remained constant or decreased slightly for all causes, noncommunicable diseases, and mental disorders overall, for anorexia nervosa and bulimia nervosa these rates increased by 6 and 10%, respectively.
Challenges to the estimation of eating disorder burden were noted by Erskine et al.[12] in 2016, for instance that ‘the representativeness of the available eating disorder prevalence data, measured as ‘coverage’, is poor’ where ‘no or limited data results in large uncertainty intervals around prevalence estimates and subsequently burden estimates’, and these still hold. Thus, GBD data on eating disorders and other mental health disorders must be interpreted with caution.
In the following two sections we look into the basic parameters for burden of disease, mortality and disability, in persons with an eating disorder as compared with persons without an eating disorder.
Mortality
Studies are reviewed that have been published since the review by Smink et al.[15] in 2013 in this journal, and which report mortality rates for eating disorder relative to a reference population: either an age-matched and sex-matched control group (death hazard ratio), or relative to expected death rates in the age-matched and sex-matched general population as a whole (standardized mortality ratio: SMR) or in the subset of the general population that has no eating disorder (mortality rate ratio: MRR). Another commonly used measure of mortality, the crude mortality rate (CMR), represents the rate of mortality within the study population (e.g. eating disorder) over a specified period. As it does not allow for comparison across study populations like the age-matched and sex-matched controlled studies do, it is not reviewed here.
In users of secondary mental healthcare services an SMR of 5.2 (95% confidence interval (CI): 3.8–7.0) was reported for anorexia nervosa and atypical anorexia nervosa according to ICD-10 criteria [16]. Also using ICD-10 criteria, Suokas et al. found a hazard ratio of 6.5 (95% CI: 3.5–12.3) for people with anorexia nervosa and atypical anorexia nervosa treated in tertiary care [17]. These rates were comparable to the SMR for anorexia nervosa of 5.9 (95% CI 4.2–8.3) calculated in a landmark meta-analysis of worldwide eating disorder mortality rates published in 2011 [18], but higher than the relative risk of 2.2 (95% CI: 2.1–2.3) for mortality of mental disorders versus controls, pooled over 148 studies [19].
One recent study, linking data from primary and secondary care, reported mortality rates for anorexia nervosa comparable to the mortality risk pooled for various mental disorders [20▪▪]: the HR for anorexia nervosa and atypical anorexia nervosa (diagnosed according to ICD-10 or Read Version 2 primary care diagnostic criteria) was 2.3 (95% CI 1.9–2.8); both genders combined. Female patients had the highest hazard ratio 2.5 (95% CI 2.1–3.1). The majority of the patients had not been referred to a hospital, and thus the eating disorders may on average have been less severe than those in previous studies, which included cases identified mainly through hospital records or eating disorder treatment facilities. In the same study, a hazard ratio of 1.4 (95% CI 1.1–1.8) was reported for bulimia nervosa and atypical bulimia nervosa, diagnosed according to ICD-10 criteria [20▪▪]. This rate is similar to the SMR of 1.5 (95% CI 1.1–2.0) of DSM-IV defined bulimia nervosa reported by Fichter and Quadflieg [21] and the SMR of 1.9 (95% CI 1.4–2.6) in the meta-analysis by Arcelus et al.[18].
In their review, Smink et al. identified one study that reported an SMR for BED of 2.3 (95% CI 0.0–5.5) [9]. Since then, two follow-up studies have reported relative mortality rates for BED: in Finnish inpatients the hazard ratio was 1.8 (95% CI 0.6–5.3) [17], and in German inpatients, the SMR was 1.5 (0.9–2.4) [21]. None of the mortality rates for BED were significantly higher than in controls.
For the combined category of anorexia nervosa, bulimia nervosa, and other eating disorders (ICD-10 code F50), in a study linking data from the Danish Psychiatric Central Research Register (containing information on inpatient treatment and outpatient and emergency room visits) with the Danish Register of Causes of Death, an overall MRR of 2.9 (95% CI 2.6–3.1) was reported [22▪].
Finally, in one male-only, 30-year follow-up study of inpatients, SMRs were 5.9 (95% CI 3.6–9.2) for anorexia nervosa, 1.9 (95% CI 0.9–3.6) for bulimia nervosa, and 3.4 (95% CI 1.4–7.0) for EDNOS; all diagnoses according to DSM-IV [23]. These results are largely in line with previous studies reporting mortality in male patients with an eating disorder.
Disability and functioning
Erskine et al.[12] extended the GBD context for disability from time lived with loss of health to a broader concept capturing deficits in other areas and the impact on caregivers and the community. This was reflected in disability weights derived from population surveys where respondents make pairwise comparisons of health conditions as to which of the two they consider the most ‘unhealthy’. On a scale of 0 (perfect health) to 1 (death), disability weights for anorexia nervosa were calculated at 0.224 and for bulimia nervosa at 0.223. These are worse (higher weights) than, for example, for chronic state kidney disease (0.104) or severe heart failure (0.179), but better than for schizophrenia (0.778), which had the highest disability weight among 301 acute and chronic diseases and injuries [24].
Disability and functioning are two sides of the same coin. The WHO International Classification of Functioning, Disability and Health (ICF) provides a framework for measuring functioning and disability in relation to health conditions [25]. The WHO Disability Assessment Schedule (WHODAS 2.0) is the associated measuring instrument and looks into psychosocial activities and participation. In DSM-5, the WHODAS 2.0 has been put forward to replace the Global Assessment of Functioning (GAF) scale used in DSM-IV [26]. The original version is patient-based. However, for patients with severe mental illness who lack insight into their health problems, Koopmans et al. [27]. advocated the use of the proxy version by a caregiver or well informed health professional.
Despite the fact that DSM-5 has been introduced in 2013, the WHODAS 2.0 has not so far been widely adopted in mental health research and practice. Although Edlund et al.[28] indicated that eating disorders ‘might be highly disabling’, in their nationally representative population surveys using the WHODAS 2.0, the authors did not include eating disorders because of their relatively low prevalence. The two studies that did assess a patient-reported version of the WHODAS in patients with an eating disorder either did not have a noneating disorder control group [29] or did not report separately on patients with an eating disorder [30]. As yet, no study has used the proxy version of the WHODAS 2.0 in people with an eating disorder. For anorexia nervosa, in particular, the proxy information may be warranted, as patients with anorexia nervosa often deny that they are ill. Furthermore, parents are an important source of information on children and adolescents, as anorexia nervosa shows a peak incidence between 12 and 19 years old [31].
Quality of life
A report commissioned by a UK national charity indicated that, according to both patients with an eating disorder and their caregivers, eating disorders had a significant impact on patients’ participation and productivity at education and work, overall well being, and quality of life, and on social and family life for both patients and their caregivers [32].
Several recent studies have reported problems in quality of life for current and former patients with an eating disorder. A general population cohort study in the USA revealed that those with a lifetime history of eating disorder (anorexia nervosa, bulimia nervosa, BED, and other eating disorder diagnoses combined) had a significantly lower quality of life (as measured with the EQ-5D-5L) than noneating disorder controls [33]. In a review of residual eating disorder symptoms and clinical features in patients who were in remission or had recovered, Tomba et al.[34▪] reported that former eating disorder patients had a significantly lower quality of life and reduced capabilities in several areas of social functioning compared with noneating disorder controls, and that psychological well being did not improve up to the level of healthy controls. De Vos et al.[35] reported that patients with anorexia nervosa, bulimia nervosa, BED or Other Specified Feeding and Eating Disorders (OSFED) had significantly worse scores than the general population on overall, emotional and psychological well being; social well being was significantly lower only for patients with anorexia nervosa and bulimia nervosa. They also looked at ‘the other side’ of the spectrum of mental health states and found that some of those with an eating disorder reported they were flourishing; ranging from 9.3% (anorexia nervosa) to 24.6% (BED) compared with 36.8% in the general population.
Comorbidity is common in eating disorders and may increase the burden of disease. A 2019 review in this journal by Rijkers et al.[36] indicated that the prevalence of PTSS in eating disorders ranged from 9 to 24%. Patients with an eating disorder (n = 6560) were reported to experience higher levels of personality disorders (odds ratio (OR) = 10.8; 95% CI 6.6–18.6), alcohol dependence syndrome (OR = 6.0, 95% CI 3.9–9.4), and depressive disorders (OR = 5.9; 95% CI 4.8–7.4) than a group of age-matched and sex-matched controls [20▪▪]. The impact of eating disorders on well being may already be visible in health service use data prior to diagnosis as indicated by increased general practitioner prescriptions for central nervous system and dietetic drugs in the 2 years before the diagnosis of an eating disorder [20▪▪].
Economic cost
Another way to look at illness burden is to consider the costs to the individual and to society. In 2005, Simon et al.[37] reviewed the health service use and cost of patients with an eating disorder. They concluded that much less was known about this topic in eating disorders than in many other mental disorders. This was still found to be the case as recently as 2019 [38]. Mental illnesses, in general, reduce the chances of completing school, getting and keeping a full-time job, and earning high wages [38]. The long-term costs of an illness may be higher when the peak age at incidence is relatively low and chronicity is high, such as in eating disorders.
Disease costs of eating disorder involve treatment costs, and direct financial burden and loss of earnings for both patients and caregivers. The BEAT report calculated direct yearly costs of eating disorders in Wales at £1500 for patients and £2800 for caregivers, and the average costs for treatment per patient at £8850 per year [32]. Yearly costs of time off work and education were found to be £650 for patients with an eating disorder under 20 years old, £9500 for those over the age of 20, and £5950 for caregivers. The loss of earnings was reported to extend beyond the average treatment period of 6 years. How these costs related to healthcare costs for people without an eating disorder was not assessed. A review by Agh et al.[39] analysed 17 studies reporting healthcare costs of eating disorders; none of these compared costs with those of noneating disorder controls. Samnaliev et al.[40] reported that people with an eating disorder in the USA had yearly healthcare costs that were on average 48% higher than in the general population, and that within those with an eating disorder who were employed, the presence of mental health comorbidity was associated with an almost 50% reduction of yearly earnings. Another study found that healthcare use and associated costs in the year prior to a diagnosis of BED were already higher than for controls [41].
Family burden
Finally, eating disorders may not only impact the person with an eating disorder, but also affect relatives, in particular caregivers (parents) and offspring as well. There are very few studies that address caregiver's burden in eating disorders, let alone compare these to other health conditions or noneating disorder controls. A comparison by Martín et al. between caregivers of patients with an eating disorder, with depression or with schizophrenia, indicated that the caregiver's burden (worrying, tension, urging) was higher for carers of patients with an eating disorder [42]. In a study on anorexia nervosa, negative perceptions of the consequences of anorexia nervosa for young people also negatively impacted the caregiver's burden, regardless of anorexia nervosa symptom severity [43].
In a small-scale longitudinal study, Martini et al.[44] found that at 6 months postpartum, mothers with current and past eating disorder reported higher concerns about their child being or becoming overweight, and were less aware of hunger and satiety cues in their child, compared with healthy controls. A systematic literature review of studies comparing mothers with and without an eating disorder and their children revealed a range of differences that indicate an impact of maternal eating disorder on the child's psychological, cognitive, and eating development, such as more behavioural difficulties regarding feeding and eating, more socioemotional difficulties, and possibly an increased risk for the development of eating disorder in the child [45]. Reports of children's difficulties by mothers with an eating disorder may be biased and need to be considered with caution.
In women from Utah, USA, with a previous eating disorder, age at first birth (anorexia nervosa: 26.4 years; bulimia nervosa: 25.7 years; EDNOS 25.6 years) was significantly higher than in matched controls from the general population (24.1 years) [46]. Taking marital status into consideration, fertility rates for anorexia nervosa were 18%, for bulimia nervosa 23.3%, and for EDNOS 18.6%, compared with 48.3% in age-matched general population controls. This indicates that women with an eating disorder history may experience delay or disruption of their reproduction because of their previous eating disorder. In Sweden, a large birth register study revealed increased risks for adverse pregnancy and neonatal outcomes, such as preterm birth and microcephaly, both for women with a current eating disorder as well as those with an eating disorder in remission [47▪].
CONCLUSION
Long-term studies showed considerable rates of persisting eating disorder pathology. This protracted eating disorder pathology means that worldwide, each year an estimated 3.3 million healthy person-years are lost to disability. Also, anorexia nervosa and bulimia nervosa are accompanied by significantly increased mortality rates. Patients with anorexia nervosa who have received inpatient treatment have higher rates than average for mental disorders. Eating disorders also negatively affect years lived with disability, the individual's quality of life, economic costs for patients and their caregivers, and childbearing and parenting. Only a few studies compare disease burden between people with and without an eating disorder, or use standardized rates for relevant data. Further eating disorder research is needed on patients’ functioning as measured with the WHODAS 2.0 introduced by DSM-5.
Acknowledgements
None.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
REFERENCES AND RECOMMENDED READING
Papers of particular interest, published within the annual period of review, have been highlighted as:
▪ of special interest
▪▪ of outstanding interest
REFERENCES
- 1.Treasure J, Duarte TA, Schmidt U. Eating disorders. Lancet 2020; 395:899–911. [DOI] [PubMed] [Google Scholar]
- 2.Svaldi J, Schmitz F, Baur J, et al. Efficacy of psychotherapies and pharmacotherapies for bulimia nervosa. Psychol Med 2019; 49:898–910. [DOI] [PubMed] [Google Scholar]
- 3.de Jong M, Schoorl M, Hoek HW. Enhanced cognitive behavioural therapy for patients with eating disorders: a systematic review. Curr Opin Psychiatry 2018; 31:436–444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Peat CM, Berkman ND, Lohr KN, et al. Comparative effectiveness of treatments for binge-eating disorder: systematic review and network meta-analysis. Eur Eat Disord Rev 2017; 25:317–328. [DOI] [PubMed] [Google Scholar]
- 5.van den Berg E, Houtzager L, de Vos J, et al. Meta-analysis on the efficacy of psychological treatments for anorexia nervosa. Eur Eat Disord Rev 2019; 27:331–351. [DOI] [PubMed] [Google Scholar]
- 6.Wonderlich SA, Bulik CM, Schmidt U, et al. Severe and enduring anorexia nervosa: update and observations about the current clinical reality. Int J Eat Disord 2020; 02:1–10. [DOI] [PubMed] [Google Scholar]
- 7.Fichter MM, Quadflieg N, Crosby RD, Koch S. Long-term outcome of anorexia nervosa: results from a large clinical longitudinal study. Int J Eat Disord 2017; 50:1018–1030. [DOI] [PubMed] [Google Scholar]
- 8▪▪.Quadflieg N, Fichter MM. Long-term outcome of inpatients with bulimia nervosa - results from the Christina Barz Study. Int J Eat Disord 2019; 52:834–845. [DOI] [PubMed] [Google Scholar]; Unique outcome study of bulimia nervosa inpatients (N = 1351), with a long-term follow-up of 11 years after admission. Also includes data on a subsample followed up for 21 years.
- 9.Fichter MM, Quadflieg N, Hedlund S. Long-term course of binge eating disorder and bulimia nervosa: relevance for nosology and diagnostic criteria. Int J Eat Disord 2008; 41:577–586. [DOI] [PubMed] [Google Scholar]
- 10.Andres-Pepina S, Plana MT, Flamarique I, et al. Long-term outcome and psychiatric comorbidity of adolescent-onset anorexia nervosa. Clin Child Psychol Psychiatry 2020; 25:33–44. [DOI] [PubMed] [Google Scholar]
- 11▪▪.Rydberg Dobrescu S, Dinkler L, Gillberg C, et al. Anorexia nervosa: 30-year outcome. Br J Psychiatry 2020; 216:97–104. [DOI] [PMC free article] [PubMed] [Google Scholar]; Exceptionally long (30 years) case--control outcome study of anorexia nervosa, based on population cohort of adolescents, with very high follow-up rate. It reflects the course of adolescent-onset anorexia nervosa.
- 12.Erskine HE, Whiteford HA, Pike KM. The global burden of eating disorders. Curr Opin Psychiatry 2016; 29:346–353. [DOI] [PubMed] [Google Scholar]
- 13▪.GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017 [published correction appears in Lancet. 2019 Jun 22;393(10190):e44]. Lancet 2018; 392:1789–1858. [DOI] [PMC free article] [PubMed] [Google Scholar]; One of the key Lancet papers on the GBD 2017, providing information on YLD for a large range of diseases, including eating disorders.
- 14. Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2017 (GBD 2017) Results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME), 2018. Available at: http://ghdx.healthdata.org/gbd-results-tool. (Accessed April 30 2020). [Google Scholar]
- 15.Smink FR, van Hoeken D, Hoek HW. Epidemiology, course, and outcome of eating disorders. Curr Opin Psychiatry 2013; 26:543–548. [DOI] [PubMed] [Google Scholar]
- 16.Himmerich H, Hotopf M, Shetty H, et al. Psychiatric comorbidity as a risk factor for mortality in people with anorexia nervosa. Eur Arch Psychiatry Clin Neurosci 2019; 269:351–359. [DOI] [PubMed] [Google Scholar]
- 17.Suokas JT, Suvisaari JM, Gissler M, et al. Mortality in eating disorders: a follow-up study of adult eating disorder patients treated in tertiary care, 1995–2010. Psychiatry Res 2013; 210:1101–1106. [DOI] [PubMed] [Google Scholar]
- 18.Arcelus J, Mitchell AJ, Wales J, Nielsen S. Mortality rates in patients with anorexia nervosa and other eating disorders. Arch Gen Psychiatry 2011; 68:724–731. [DOI] [PubMed] [Google Scholar]
- 19.Reisinger Walker E, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiatry 2015; 72:334–341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20▪▪.Demmler JC, Brophy ST, Marchant A, et al. Shining the light on eating disorders, incidence, prognosis and profiling of patients in primary and secondary care: national data linkage study. Br J Psychiatry 2019; 216:105–112. [DOI] [PMC free article] [PubMed] [Google Scholar]; This study used linked electronic health records from general practices and hospital admissions nationwide. Data from eating disorder cases and controls in the 2 years before and 3 years after diagnosis were analysed, providing important insights into healthcare use and the associated costs preceding and following diagnosis.
- 21.Fichter MM, Quadflieg N. Mortality in eating disorders - results of a large prospective clinical longitudinal study. Int J Eat Disord 2016; 49:391–401. [DOI] [PubMed] [Google Scholar]
- 22▪.Plana-Ripoll O, Pedersen CB, Agerbo E, et al. A comprehensive analysis of mortality-related health metrics associated with mental disorders: a nationwide, register-based cohort study. Lancet 2019; 394:1827–1835. [DOI] [PubMed] [Google Scholar]; Comprehensive analysis of mortality of different types of mental disorders, displayed by age, sex, and cause of death, in a 10-year population cohort (N = 7 369 926; 111 027 388 person-years).
- 23.Quadflieg N, Strobel C, Naab S, et al. Mortality in males treated for an eating disorder - a large prospective study. Int J Eat Disord 2019; 52:1365–1369. [DOI] [PubMed] [Google Scholar]
- 24.Global Burden of Disease Study 2013 Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015; 386:743–800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.World Health Organization ICF: International Classification of Functioning, Disability and Health. Geneva: WHO; 2001. [Google Scholar]
- 26.American Psychiatric Association Diagnostic and statistical manual of mental disorders (5th ed.; DSM-5). Washington, DC: Author; 2013. [Google Scholar]
- 27.Koopmans AB, van Hoeken D, Clarke DE, et al. Proxy WHO Disability Assessment Schedule 2.0 is clinically useful for assessing psychosocial functioning in severe mental illness. Front Psychiatry 2020; 11:303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Edlund MJ, Wang J, Brown KG, et al. Which mental disorders are associated with the greatest impairment in functioning? Soc Psychiatry Psychiatr Epidemiol 2018; 53:1265–1276. [DOI] [PubMed] [Google Scholar]
- 29.Preti A, Girolamo Gd, Vilagut G, et al. The epidemiology of eating disorders in six European countries: results of the ESEMeD-WMH project. J Psychiatr Res 2009; 43:1125–1132. [DOI] [PubMed] [Google Scholar]
- 30.Sedano-Capdevila A, Barrigon ML, Delgado-Gomez D, et al. WHODAS 2.0 as a measure of severity of illness: results of a FLDA analysis. Comput Math Methods Med 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Steinhausen HC, Jakobsen H. Incidence rates of treated mental disorders in childhood and adolescence in a complete nationwide birth cohort. J Clin Psychiatry 2019; 80: 17m12012. [DOI] [PubMed] [Google Scholar]
- 32. Beat. The cost of eating disorders; social, health and economic impacts. 2015. Available at: https://www.beateatingdisorders.org.uk/uploads/documents/2017/10/the-costs-of-eating-disorders-final-original.pdf. Accessed at April 29 2020. [Google Scholar]
- 33.Hart LM, Gordon AR, Sarda V, et al. The association of disordered eating with health-related quality of life in U.S. young adults and effect modification by gender. Qual Life Res 2020; 29:1203–1215. [DOI] [PubMed] [Google Scholar]
- 34▪.Tomba E, Tecuta L, Crocetti E, et al. Residual eating disorder symptoms and clinical features in remitted and recovered eating disorder patients: a systematic review with meta-analysis. Int J Eat Disord 2019; 52:759–776. [DOI] [PubMed] [Google Scholar]; A systematic review with meta-analyses of residual eating disorder symptoms and associated noneating disorder clinical features. It offers a broad perspective on impairments and deficits associated with eating disorders.
- 35.de Vos JA, Radstaak M, Bohlmeijer ET, Westerhof GJ. Having an eating disorder and still being able to flourish? Examination of pathological symptoms and well being as two continua of mental health in a clinical sample. Front Psychol 2018; 9:2145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Rijkers C, Schoorl M, van Hoeken D, Hoek HW. Eating disorders and posttraumatic stress disorder. Curr Opin Psychiatry 2019; 32:510–517. [DOI] [PubMed] [Google Scholar]
- 37.Simon J, Schmidt U, Pilling S. The health service use and cost of eating disorders. Psychol Med 2005; 35:1543–1551. [DOI] [PubMed] [Google Scholar]
- 38.Doran CM, Kinchin I. A review of the economic impact of mental illness. Aust Health Rev 2019; 43:43–48. [DOI] [PubMed] [Google Scholar]
- 39.Agh T, Kovacs G, Supina D, et al. A systematic review of the health-related quality of life and economic burdens of anorexia nervosa, bulimia nervosa, and binge eating disorder. Eat Weight Disord 2016; 21:353–364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Samnaliev M, Noh HL, Sonneville KR, Austin SB. The economic burden of eating disorders and related mental health comorbidities: an exploratory analysis using the U.S. Medical Expenditures Panel Survey. Prev Med Rep 2015; 2:32–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Watson HJ, Jangmo A, Smith T, et al. A register-based case-control study of healthcare utilization and costs in binge-eating disorder. J Psychosom Res 2018; 108:47–53. [DOI] [PubMed] [Google Scholar]
- 42.Martín J, Padierna A, van Wijngaarden B, et al. Caregivers consequences of care among patients with eating disorders, depression or schizophrenia. BMC Psychiatry 2015; 15:124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Matthews A, Lenz KR, Peugh J, et al. Caregiver burden and illness perceptions in caregivers of medically hospitalized youth with anorexia nervosa. Eat Behav 2018; 29:14–18. [DOI] [PubMed] [Google Scholar]
- 44.Martini MG, Taborelli E, Schmidt U, et al. Infant feeding behaviours and attitudes to feeding amongst mothers with eating disorders: A longitudinal study. Eur Eat Disord Rev 2019; 27:137–146. [DOI] [PubMed] [Google Scholar]
- 45.Martini MG, Barona-Martinez M, Micali N. Eating disorders mothers and their children: a systematic review of the literature. Arch Womens Ment Health 2020; 10.1007/s00737-020-01019-x 10.1007/s00737-020-01019-x. (Accessed April 29, 2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Tabler J, Utz RL, Smith KR, et al. Variation in reproductive outcomes of women with histories of bulimia nervosa, anorexia nervosa, or eating disorder not otherwise specified relative to the general population and closest-aged sisters. Int J Eat Disord 2018; 51:102–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47▪.Mantel Ä, Lindén Hirschberg A, Stephansson O. Association of maternal eating disorders with pregnancy and neonatal outcomes [published online ahead of print, 2019 Nov 20] [published correction appears in JAMA Psychiatry. 2020 Jan 2]. JAMA Psychiatry 2019; 77:285–293. [DOI] [PMC free article] [PubMed] [Google Scholar]; First study of the association of eating disorders with pregnancy complications and neonatal health. Results indicate the need for increased surveillance in antenatal and delivery care for women with current or former eating disorders.