

Background
Arthritis is a leading cause of pain, disfigurement, and disability in the United States where nearly one quarter of all adults have received an affirmative diagnosis. [2] While the incidence of rheumatoid arthritis has remained constant, osteoarthritis (OA) diagnoses have tripled since 2000 due to an aging population, increasing levels of obesity, and greater physician recognition of its prevalence. Accordingly, OA is a leading cause of chronic pain and disability among the elderly. [23] Irrespective of the precipitating cause, the pathology of joint destruction in arthritis is driven by an overlapping profile of pathologic inflammatory cytokines including TNF-α, IL-1β, IL-6, IL-17, and IL-21. [26; 46; 49] Additionally, pain, inflammation, and joint destruction among both etiologies are mediated by overlapping subsets of innate cell types including neutrophils. [16; 45] Treatment of rheumatoid arthritis consists of both targeted and non-specific immunosuppressive drug regimens (DMARDs or disease-modifying antirheumatic drugs) whereas treatment of OA consists of analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), glucocorticoids, and joint replacement supplemented by a weight loss regimen, if applicable. In either case, pharmacomodulation is not curative and often accompanied by severe side-effects. [6; 9; 36] Because pain is the predominant symptom of OA, it is also the primary target of intervention. Recent reviews comparing the efficacy of pharmacotherapies for reducing OA pain conclude opioids are most effective, though abuse potential limits utility. Overall the effective size across all pharmacotherapies is small (0.39), signaling a need for additional treatments with novel and complementary mechanisms of action. [1; 32; 54; 61]
The ubiquitous endocannabinoid system (ECS) plays a role in many physiological and pathophysiological processes. Consistent with this, cannabis and its constituents are increasingly being recognized as bona fide pharmacologic agents with significant therapeutic potential. For example, cannabidiol (CBD), the major non-THC constituent of cannabis, can exert numerous biological effects through several different receptors and signaling pathways, including anti-inflammatory effects in both acute and chronic conditions. [10–13; 20; 25; 43; 47; 51; 57] Indeed, preclinical rodent models suggest the therapeutic potential of CBD in combating the underlying causes of both rheumatoid arthritis and OA. [15; 35; 37; 48]
While preclinical rodent models have provided evidence of efficacy for novel compounds to treat pain [8; 19; 29], the clinical efficacy or safety of these compounds in human studies has been unsatisfying. [58; 59] The late-stage failures of promising compounds in randomized studies have suggested a disconnect between the preclinical models used to study structural versus symptomatic aspects of disease. [17] Indeed, the initiating event and many of the pathological changes in the commonly used, chemically-induced preclinical rodent models of chronic OA pain are not typical of human OA. [17; 56] In contrast, spontaneous models, particularly domesticated canine models, are more appropriate for assessing OA pain treatments because they closely mimic the pathophysiology and pathogenesis of human OA pain. [17] In the present work, we determined the in vitro and in vivo effects of CBD on expression levels of shared, pathologic pro-inflammatory cytokines and innate cell subsets in multiple model systems. Subsequently, the safety and efficacy of CBD were evaluated in a double-blind, placebo-controlled study in a spontaneous canine model.
Methods
Cannabidiol (CBD).
CBD, provided by MedterraCBD (Irvine, CA), was isolated solely from hemp grown and extracted under the strict guidelines of the Kentucky Department of Agricultural Industrial Hemp pilot program. Subsequent analysis by third party (ProVerde Laboratories, Milford, MA) mass spectrometry confirmed the absence of Δ9-tetrahydrocannabinol (THC), other cannabinoid derivatives, and contaminants while further HPLC testing demonstrated CBD isolate purity of 99.9%. For all assays, CBD was solubilized in fractionated coconut oil. Liposomal CBD was produced using a sunflower lecithin (phosphatidyl choline) base. Each liposome was approximately 100 nm, allowing encapsulation of 10–20 mg/ml CBD. Transmission Electron Microscopy (TEM) was used to observe and confirm the stability of liposomal CBD concentration, size, and polydispersity following storage at 4°C for at least 3 months. Briefly, samples were placed on 150 mesh formvar coated copper grids treated with poly-l-lysine for approximately 1 hour, then negatively stained with filtered aqueous 2% ammonium molybdate + 0.02% BSA, pH 7.0 for 1 min. Stain was blotted dry from the grids with filter paper and samples were allowed to dry. Samples were then examined in a JEM 1010 transmission electron microscope (JEOL USA, Peabody, MA) at an accelerating voltage of 80 Kv. Digital images were obtained using the AMT Imaging System (Advanced Microscopy Techniques Corp., Danvers, MA).
Cell culture.
Mouse RAW267.4 macrophage cells (ATCC, Manasas, VA), primary mouse splenocytes, human monocytic THP-1 cells (ATCC), and human PBMC were plated in a single well of a 6-well plate in 5 ml RPMI (Invitrogen, Carlsbad, CA) medium supplemented with 10% fetal bovine serum at 5% CO2 in a 37°C humidified incubator for either 2 (lipopolysaccharide; LPS) or 4 hours (staphylococcal enterotoxin B; SEB) before addition of CBD. LPS and SEB concentrations employed were determined by previous publications and empirical testing per cell culture. TNF-⍺ levels in cell culture supernatants were determined using the TNF Flex Set immunoassay (BD Biosciences, San Jose, CA) as measured by an LSR II or Canto Violet flow cytometer (BD Biosciences) and analyzed with FlowJo version 10.0.00003 (Tree Star, Inc., Ashland, OR). All points were assayed in triplicate with at least three independent repetitions unless stated otherwise.
Mice.
Approximately 342 female, 6–10 week old C57BL/6J mice with a weight range of 18 to 27 grams were procured from Baylor College of Medicine or the Jackson Laboratory (Bar Harbor, ME) and maintained in accordance with the specific IACUC requirements of Baylor College of Medicine and in accordance with animal protocol AN-7942. Mice were housed under controlled standard conditions (23 +/− 1°C, 55 +/− 10% humidity and a 12-h light/dark cycle) and provided standard laboratory chow and autoclaved water ad libitum.
Croton oil-induced ear inflammation model.
All experiments were conducted between 10 a.m. and 3 p.m., in order to avoid the influence of circadian variations in corticosteroid levels in the murine inflammatory response. Croton oil (2.5% in acetone) was topically applied (100 μl) to the right ear. Two hours after croton oil was applied, vehicle or 100 μl of 10mg/ml CBD oil was topically applied to swollen and control ears. Two hours after these treatments, ear tissue samples were collected to determine MPO activity and blood samples were collected by retro-bleed to determine circulating TNF-⍺ levels.
LPS-Induced inflammation model.
LPS (200 ng) was administered intraperitoneally. Two hours after LPS administration, mice were injected intraperitoneally with CBD (1, 10 or 100 μg) or administered either CBD (100 μg) or 18.3% methyl salicylate/16% menthol (Ben-Gay, Johnson & Johnson, New Brunswick, NJ) topically at the LPS injection site. Two hours after treatments, blood samples were collected by retro-bleed to determine cytokine and neutrophil levels.
Tissue MPO activity.
In brief, ear tissue samples (4 mm punch) collected at 1, 2, 3, or 4 hours after croton oil was applied were homogenized in MPO assay buffer (Abcam, Cambridge, MA) per the manufacturer’s instructions. Samples and MPO assay buffer were equilibrated to room temperature before use, and samples were diluted 1:5 in assay buffer. Groups were assayed in triplicate in individual wells in 50 μl of reaction mix for 2 hrs at room temperature before addition of 2 μl of stop mixture. Subsequently, 50 μl of TMB developer substrate was added and incubated for 10 min, and the output was measured by spectrophotometry at OD412 nm.
Cytokine and neutrophil analysis.
Mice were bled retro-orbitally at specified intervals. Blood samples were mixed with 0.5M EDTA to prevent clotting then pelleted to extract the serum. Red blood cells in the cell pellet were lysed by suspension in ammonium chloride (Sigma-Aldrich, St. Louis, MO) per the manufacturer’s instructions. The remaining white blood cells were then stained for neutrophils by CD45-APC-Cy7, CD11b-APC, Ly6G-FITC, and CD115-PE (all from BioLegend, San Diego, CA) before analysis by flow cytometry. The serum was subsequently analyzed for various cytokines using the BD flex set (BD Biosciences). In brief, the serum was diluted with supplied buffer per manufacturer’s instructions, incubated with the appropriate capture antibody/bead for 1 hr at room temperature, incubated with the detection antibody/bead for another hour at room temperature, washed, centrifuged, resuspended in flow buffer, and analyzed by flow cytometry.
Bioluminescence imaging.
Mice were subcutaneously injected with 5 × 105 luc2+ KRAS tumor cells near the hindquarters 24 hrs prior to experimentation. Subsequently, mice were subcutaneously injected with 100 μl either 10 mg/ml naked D-luciferin (Regis Technologies, Morton Grove, IL) or 10 mg/ml liposomally-encapsulated D-luciferin near the forequarters on the ipsilateral side. Mice were then analyzed continuously be IVIS imaging (Caliper Life Sciences, Waltham, MA) for 2 hrs.
Human subjects bioavailability trial design.
A longitudinal crossover study to compare the bioavailability of liposomal vs. naked CBD was approved and carried out under an IRB-approved protocol under the auspices and guidance of the Institute for Regenerative and Cellular Medicine (IRCM, Santa Monica, CA). Following provision of informed consent, subjects were randomized regarding the order of which to receive an isolate of either naked CBD or liposomally-encapsulated CBD. At first study visit, peripheral blood was drawn following overnight fasting to measure the baseline cannabidiol (CBD) blood levels. Subjects then orally ingested an amount of isolate equivalent to 10 mg CBD in either naked or liposomally-encapsulated form. One hour after the product was ingested, a second blood draw was taken to determine circulating levels of CBD. Two weeks later at the second study visit, the same procedure was followed with the exception that the study subject was administered the converse form of delivery not received at the first study visit. Subjects were eligible for inclusion if a) between the ages of 25 and 70, b) able to read and sign the informed consent and stay compliant with study requirements and schedule, c) not taking any other CBD product concurrently, and d) in good general health. Patients with terminal illnesses were prohibited from study participation. Bioavailability ratio of liposomally-encapsulated CBD to naked CBD administration was calculated using an LOQ value of 0.05 ng/ml (limit of detection) if naked CBD administration produced undetectable levels of circulating CBD.
Osteoarthritis veterinary trial design.
Canine veterinary studies were performed with oversight as stipulated by Baylor College of Medicine IACUC protocol AN-7705. The study population consisted of client-owned dogs presenting to Sunset Animal Hospital (Houston, TX) for evaluation and treatment of lameness due to OA. Owners completed a brief questionnaire to define the affected limb(s), duration of lameness, and duration of analgesic or other medications taken. Dogs were considered for inclusion in the study if they 1) received an affirmative diagnosed of OA by a veterinarian and 2) demonstrated signs of pain according to assessment by their owners, detectable lameness on visual gait assessment, and painful joint(s) upon palpation. Complete blood count (CBC) and serum chemistry were performed at presentation to rule out other underlying disease. Dogs were excluded by the attending study veterinarian if they exhibited evidence of uncontrolled renal, endocrine, neurologic, or neoplastic disease, or were undergoing physical therapy. No cases of OA were related to trauma, and no animals with end-stage disease were enrolled. All other medications were discontinued at least 2 weeks prior to enrollment and dogs were not allowed to receive any medications during the 4-week study period except the study medication. Large (> 20 kg, mean 41 +/− 15 kg) domestic canines were enrolled in the 4-week, randomized placebo-controlled trial in which both owner and veterinarian were blinded. Following provision of informed owner consent, 20 study subjects were randomly assigned 1:1:1:1 to 1 of 4 groups: placebo, 20 mg/day (0.5 mg/kg) naked CBD, 50 mg/day (1.2 mg/kg) naked CBD, or 20 mg/day liposomal CBD. Simple randomization was achieved by providing the blinded study drug regimens to the veterinary investigator in a randomized numerical order labeled 1 to 20 as assigned by the rolling of a die. Following randomization, aggregate average weight of each study group remained within one standard deviation of all other study groups. Blood was collected for CBC and clinical chemistry at initiation and at day 30 of treatment. Before treatment initiation and at day 30, each dog was evaluated by the study veterinarian who assessed locomotion as it related to walking, running, and assuming a standing position from both a sitting and lying down position on a 5-point scale (1 = best) during physical examination. Owners also evaluated dogs before treatment and at weeks 4 and 6 using the Helsinki Chronic Pain Index (HCPI), a validated, 11-item assessment of treatment response in dogs with OA pain scored ordinally on a scale from 0 to 4. [18]
Statistical analysis.
Data are expressed as the mean ± SD unless otherwise specified. Student’s t-test was used for pairwise comparisons, and one-way ANOVA followed by post-hoc Tukey–Kramer was used for analysis of multiple comparisons. Normality of data was determined by Q-Q plot. Statistical significance was defined as p < 0.05 unless stated otherwise. Sample sizes for mouse, canine, and human experiments were based upon power analysis indicating that a difference in mean value (Δμ) as small as 0.25-fold could be detected with a power of 0.8 and type I error rate (α) of 0.05 with a sample size of four subjects assuming a standard deviation (σ) of 0.33. Given this calculation, we chose a sample size of five subjects for all experimental groups to permit even greater statistical discernment power (< Δμ of 25%) and/or to accommodate greater variance (σ > 1/3 SD) between groups.
Results
CBD reduces pro-inflammatory TNF-α secretion in vitro.
It has been widely reported that CBD possesses significant anti-inflammatory properties in a variety of different experimental systems. [27] To validate that the CBD used for these studies might potentiate anti-inflammatory effects relevant to arthritis, two different inflammatory stimuli were applied to four different relevant cell populations including a mouse monocyte cell line, a human monocyte cell line, primary mouse PBMC, and primary human PBMC. As illustrated in Fig 1, both lipopolysaccharide (LPS) and staphylococcus enterotoxin B (SEB) induced log-fold elevations in TNF-α secretion in comparison to untreated or CBD-only treated controls from RAW267.4 mouse cells, primary mouse PBMC, THP-1 human cells, and primary human PBMC. However concurrent application of 100 ng/ml CBD in conjunction with LPS treatment induced a 42% (primary human PBMC) to 97% (human THP-1 cells) reduction in TNF-α secretion. Similarly, concurrent application of 100 ng/ml CBD in conjunction with SEB treatment induced a 55% (RAW267.4 mouse cells) to 63% (human THP-1 cells) reduction in TNF-α secretion (Fig 1A–D, *p<0.05 or **p<0.01).
Figure 1. CBD reduces hallmarks of arthritis-related inflammation in vitro.

5 × 106 cells of the specified type were plated in triplicate in 6-well plate in 5 ml RPMI + 10% FBS followed by addition of either 1 ng/ml LPS for 4 hrs or 100 ng/ml SEB for 6 hrs with or without the addition of 100 ng/ml CBD after 2 hrs. After the incubation period, the media was analyzed using the BD TNF-⍺ Flex set. A. TNF-⍺ levels in murine RAW267.4 macrophage cell line. B. TNF-⍺ levels in primary mouse splenocytes. C. TNF-⍺ levels in human THP-1 monocyte cell line. D. TNF-⍺ levels in primary human PBMC. Representative experiment of three shown. Error bars +/− SD. *p<0.05, **<0.01 by Student’s two-tailed t-test for all A-D. Cohorts of female mice were also treated on one ear with 100 μl 2% croton oil-acetone, and ear edema was allowed to occur for 1 – 4 hrs. At 2 hrs, mice were treated on the swollen ear with either 100 μl of vehicle or 100 μl of 10 mg/ml CBD oil. Additionally, a group of untreated mice also received 100 μl CBD-oil E. At each time point indicated, 4 mm biopsies from the most central portion of swelling was obtained, homogenized, and measured for myeloperoxidase (MPO) activity via ELISA. F. After 4 hrs, each cohort was retro-orbitally bled for analysis of circulating TNF-⍺ concentrations via the BD TNF⍺ Flex set. Each cohort consisted of n=5 mice. Representative experiment of three shown. Error bars +/− SD. *p<0.05 by Student’s two-tailed t-test.
CBD induces broad anti-inflammatory effects in vivo.
Encouraged by the in vitro data, we next employed two different mouse inflammatory models to analyze the impact of CBD on local and systemic inflammation in vivo. We first employed the croton oil model in which topical administration of croton oil to the ear of a mouse induces an inflammatory reaction that includes edema, erythema, neutrophil influx, and the production of pro-inflammatory TNF-⍺. [28] Two hours after application of 2.5% croton oil +/− topical application of 1 mg CBD, local myeloperoxidase (MPO) activity (a proxy for neutrophil influx) was measured. As indicated in Fig 1E, MPO activity in the treated ear was reduced over 80% (*p<0.05) with concurrent application of CBD. Four hours after croton oil application, levels of circulating TNF-α were assessed. As shown in Fig 1F, circulating TNF-α was decreased by 50% among mice to which croton oil + CBD had been applied in comparison to croton oil alone (*p<0.05). CBD treatment also significantly reduced the development of edema.
When administered intraperitoneally, LPS induces an inflammatory response that includes increased expression of pro-inflammatory TNF-α and IL-6, two cytokines relevant to the pathogenesis of arthritis. In this model system, 200 ng of LPS was administered i.p. Two hours later, mice were then treated i.p. with increasing doses of CBD (1, 10, or 100 μg) or topically with a single CBD dose of 100 μg. After an additional two hours, the impact of CBD treatment on circulating cytokine levels was assessed. As indicated, i.p. administration of CBD reduced circulating TNF-α and IL-6 levels in a dose responsive fashion, and 100 μg of topically applied CBD generated an anti-inflammatory effect similar to that of 100 μg injected i.p. (Fig 2A/B). Interestingly, systemic administration of CBD alone increased levels of anti-inflammatory IL-10 in the absence of inflammatory stimulus, an effect that was significantly potentiated in the presence of LPS (Fig 2C). Application of 18.3% methyl salicylate/16% menthol (Ben-Gay) made no significant impact upon any of these cytokine concentrations. In contrast to alterations in pro- and anti-inflammatory cytokine levels, significant changes to circulating neutrophil chemoattractants CXCL1 (KC) and CXCL2 (MIP-2) were not observed (Fig 2D/E). Nonetheless, circulating neutrophil levels were reduced up to 60% among LPS-treated mice to which CBD had been administered (Fig 2F).
Figure 2. Intraperitoneal CBD administration reduces inflammatory cytokines and circulating neutrophils in an in vivo LPS inflammatory model.
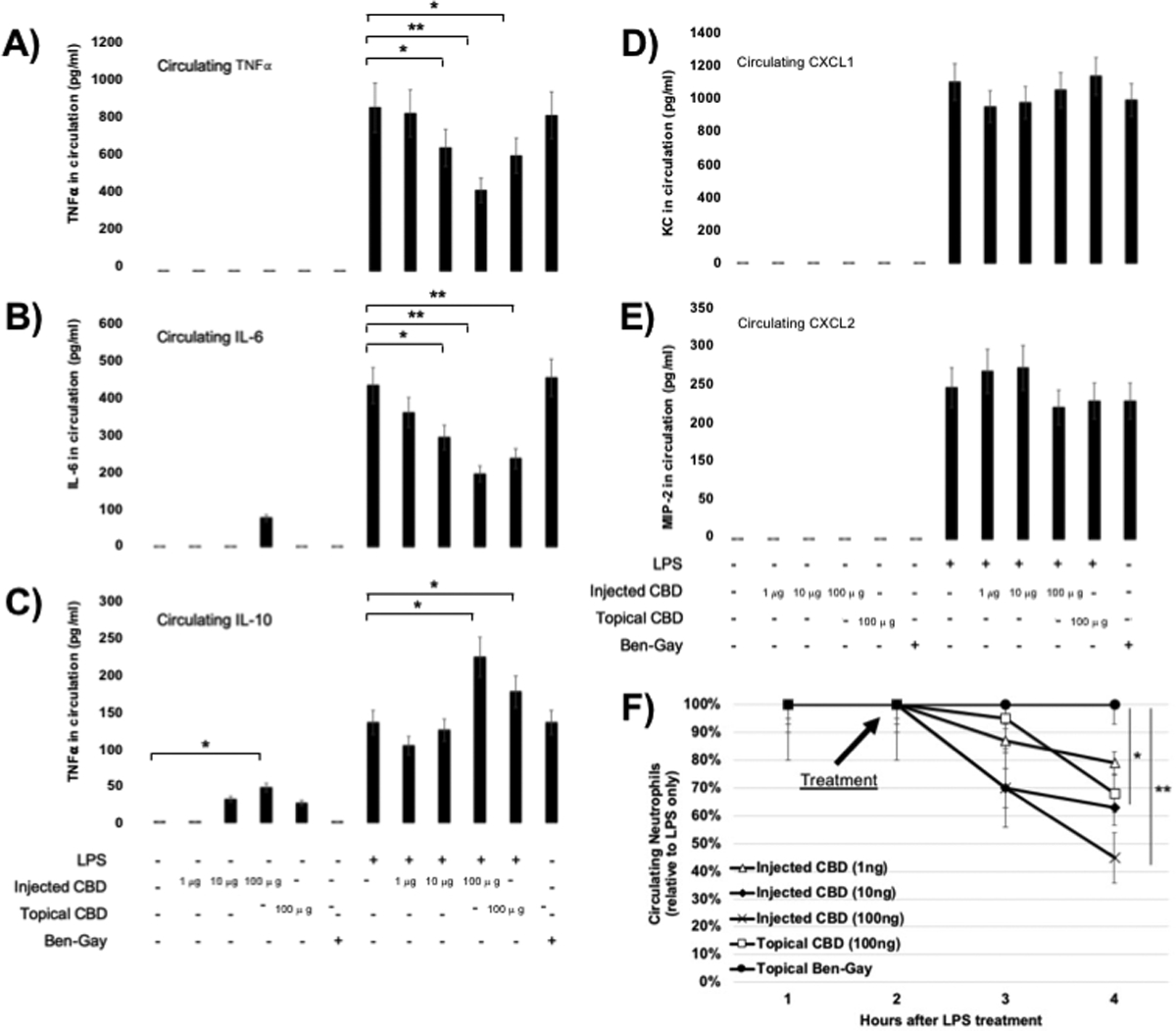
Cohorts of female mice were treated intraperitoneally with 200 ng LPS for 2 hrs and subsequently administered intraperitoneal CBD, intraperitoneal PBS control, topical CBD, or topical Ben-Gay control as indicated. After an additional 2 hours, mice were retro-orbitally bled and circulating cytokines were analyzed with the appropriate BD Flex set. A. TNF-α. B. IL-6. C. IL-10. D. CXCL1. E. CXCL2. F. Flow cytometry analysis of the cellular portion was performed each hour to determine relative number of neutrophils (CD115neg CD11b+ Ly6G+) in circulation. Representative experiment shown. Error bars +/− SD. *p<0.05, **<0.01 by one-way ANOVA.
Liposomal packaging of CBD enhances bioavailability in vivo.
Though CBD clearly displayed a role in regulating inflammation in both in vitro and in vivo murine models, the relatively low bioavailability of this hydrophobic molecule when administered orally may reduce its effectiveness. To potentially improve absorption of hydrophobic CBD isolate, we packaged it within liposomes, a vehicle delivery system previously shown to improve uptake of other hydrophobic compounds. [30] Using sunflower lecithin as a base, phosphatidylcholine liposomes approximately 100 nm in diameter and loaded with 10–20 mg/ml CBD were produced. Electron microscopy demonstrated that liposomal CBD was stable at both room temperature and 4°C and between pH 5–9 for a period of 3 months (Fig 3A).
Figure 3. Liposomal encapsulation of small molecules enhances bioavailability.

Sunflower lecithin (phosphatidyl choline) was used as a base to make liposomes approximately 100 nm in size that could encapsulate small molecules at a concentration of 10–20 mg/ml and retain polydispersity and size for at least 3 months at 4°C. A. Stable size and polydispersity observed by Transmission Electron Microscopy (TEM). B. Cohorts of mice were implanted subcutaneously injected with 500,000 luc2+ cells near the hindquarters. B/C. Twenty-four hours later, D-luciferin (100 μl, 10 mg/ml) or D-luciferin liposomes (100 μl, 10 mg/ml) was applied subcutaneously near the forequarters, and animals were continually imaged by IVIS for 2 hrs with subsequent photon measurement at the target serving as a proxy for absorption and bioavailability. D. The ability of liposomal CBD to reduce TNF-⍺ production relative to controls and naked CBD was determined. For B and C, n=5 mice per cohort. Representative experiment of three shown. For D, n=8 mice per cohort. Representative experiment of two shown. Error bars +/− SD. *p<0.05, **p<0.01 by Student’s two-tailed t-test.
To compare the bioavailability of molecules encapsulated within this liposomal containment system to that of naked molecules, we developed a proof-of-principle system utilizing liposomally-encapsulated D-luciferin and a luciferase expressing tumor cell line. In this assay system, 5 × 105 luc2+ tumor cells were implanted s.c. near the hindquarters of C57BL/6 mice. Twenty-four hours later, D-luciferin (100 μl @ 10 mg/ml) or liposomally-encapsulated D-luciferin (100 μl @ 10 mg/ml) were administered s.c. near the forequarters. Luminescence was then monitored for a continuous two-hour time period by IVIS with post-hoc photon measurement at the target serving as a proxy for substrate absorption into circulation and bioavailability. As shown in Figs 3B and 3C, liposomal packaging of D-luciferin significantly enhanced both the speed and magnitude at which this substrate was able to reach the tumor site and induce photon emission, resulting in a full log-fold enhancement of peak emissions at 60 minutes after D-luciferin administration (*p<0.05, **p<0.01 for time points indicated). Next, employing the LPS acute inflammatory model, 200 ng LPS was administered i.p., and circulating TNF-⍺ was assayed every 30 minutes and plotted as a percentage of pre-administration TNF-⍺. Two hours after introduction of LPS, mice were orally gavaged with 100 μl 10 mg/ml CBD, 10 mg/ml liposomal CBD, 10 mg/ml liposomal D-luciferin, or PBS. As shown in Fig 3D, orally administered liposomal CBD began to significantly reduce rising TNF-α levels within an hour of administration whereas an additional hour was required before orally administered naked CBD significantly reduced rising TNF-α levels in comparison to negative controls. Moreover, while both naked and liposomally-encapsulated CBD administered orally significantly reduced relative levels of circulating TNF-⍺ below those of the negative controls, liposomally-encapsulated CBD made a significantly greater impact upon such levels (*p<0.05, **p<0.01 at 4 hours after CBD administration).
Encouraged by these data, we sought to validate enhanced bioavailability of liposomally-encapsulated CBD in healthy human volunteers under the auspices of an IRB-approved and monitored human crossover study. In brief, after provision of informed consent, healthy human volunteers were randomized to receive 10 mg oral CBD in either a naked or liposomally-encapsulated formulation. Circulating CBD levels were determined from pre- and 1 hour post-administration blood draws. At a second study visit, this procedure was repeated in the same volunteer using the converse delivery method (i.e. naked vs. liposomally-encapsulated), and a bioavailability ratio was calculated. For instances in which naked CBD administration produced undetectable levels of circulating CBD, the bioavailability ratio was calculated using an LOQ value of 0.05 ng/ml (limit of detection). Among the five study volunteers for whom data were available, the bioavailability of liposomally-encapsulated CBD was 17.1 +/− 16-fold greater than that of naked CBD at one-hour post administration (*p<0.05). Further, while 2 of 5 subjects exhibited undetectable circulating CBD levels following oral administration of naked CBD isolate, all 5 subjects exhibited detectable levels of circulating CBD levels following oral administration of liposomally-encapsulated CBD (Table 1).
Table 1.
Naked vs. Liposomally-Encapsulated Circulating CBD Levels in Healthy Volunteers
| Naked CBD | Liposomal CBD | ||||
|---|---|---|---|---|---|
| Subject | Pre (ng/ml) | Post (ng/ml) | Pre (ng/ml) | Post (ng/ml) | Ratio |
| 1 | 0.00 | 0.87 | 0.00 | 5.90 | 6.8 |
| 2 | 0.00 | 0.00 | 0.00 | 0.87 | 17.4 |
| 3 | 0.00 | 0.14 | 0.10 | 2.00 | 13.6 |
| 4 | 0.00 | 0.00 | 0.19 | 2.40 | 44.2 |
| 5 | 0.00 | 0.45 | 0.00 | 1.60 | 3.6 |
| Averages | 0.29+/−0.37 | 2.55+/−1.95 | 17.1+/−16.1 | ||
Short-term administration of CBD to domestic canines diagnosed with osteoarthritis is safe and improves quality of life.
While there exist a variety of different pre-clinical mouse models of arthritis, as noted these model chemical and pathologic features of the disease have been poorly predictive in determining symptomatic or therapeutic responses. [17] In an effort to better model treatment efficacy, we conducted a randomized, double blind, placebo-controlled trial among large (> 20 kg; mean = 41 +/− 15 kg) outbred canines with an affirmative veterinary diagnosis of osteoarthritis and experiencing decreased mobility and quality of life. Following diagnosis and provision of owner informed consent, animals were enrolled and randomly provided with identical medication bottles which contained one of four treatments including 10 mg/ml naked CBD, 25 mg/ml naked CBD, 10 mg/ml liposomal CBD, or a placebo consisting only of fractionated coconut oil. Baseline and day 30 CBC and metabolic panel as well as alanine aminotransferase (ALT) and alkaline phosphatase (ALKP) were also determined. Symptomology was assessed by the attending study veterinarian through clinical examination on days 0 and 30 and by each animal’s owner on study days 0, 30, and 45 using the Helsinki Chronic Pain Index (HCPI) assessment. [18] Characteristics of each enrolled animal are provided in Supplementary Table 1. As shown in Fig 4A/B, owner assessment of animal symptomology was not significantly altered by administration of placebo or 20 mg/day naked CBD; however, administration of 50 mg/day naked CBD or 20 mg/day liposomal CBD generated statistically significant reductions in pain symptomology (**p<0.01), an effect that remained statistically significant (*p<0.05) for at least 15 days after cessation of therapy. With some variability, veterinarian clinical examination largely matched that of the owners assessment with generally no improvements observed among animals administered placebo or 20 mg/day naked CBD, and significant improvements noted among all four assessment categories (sitting to standing, lying to standing, walking, running) among dogs who received 50 mg/day naked CBD and 20 mg/day liposomal CBD as evidenced by group compilation raw assessment scores (Fig 5A–D) or a secondary analysis (Fig 6) that considered only whether symptomology in a given study participant worsened, remained the same, or improved over the course of therapy (*p<0.05, **p<0.01, ****p<0.001). No sex differences with regard to treatment efficacy were observed, and there were no significant alterations to CBC, metabolic panel, or ALT/ALKP values over the course of the study in any group (Fig 7A–C and Table 2).
Figure 4. Daily administration of CBD for 30 days improves owner-perspective QOL scores among large dogs with affirmative diagnosis of osteoarthritis.

Twenty large domestic canines with affirmative diagnosis of osteoarthritis were enrolled in a double-blind, placebo-controlled randomized study. animals were administered coconut oil placebo, 20 mg/day naked CBD, 50 mg/day naked CBD, or 20 mg/day liposomal CBD. Owners assessed their animals by means of the Helsinki Chronic Pain Index (HPCI) on days 0, 30, and 45. A. Individual HPCI values were plotted for each study cohort on days 0 and 30. B. Cohort HPCI values were plotted on days 0, 30, and 45. Error bars +/− SD. *p<0.05, **p<0.01 by Student’s two-tailed t-test.
Figure 5. Daily administration of CBD for 30 days improves veterinarian-perspective subset QOL scores among large dogs with affirmative diagnosis of osteoarthritis.

Study enrolled canine subjects were scored by the (blinded) study veterinarian on days 0 and 30 using a scale of 1 (best) to 5 (worst) for four different movements consisting of sitting to standing, lying to standing, walking, and running. Subset scale data comparing day 0 and day 30 scores for each task are shown by cohort. Error bars +/− SEM. *p<0.05, **p<0.01 by Student’s two-tailed t-test.
Figure 6. Daily administration of CBD for 30 days improves veterinarian-perspective overall QOL scores among large dogs with affirmative diagnosis of osteoarthritis.

Study enrolled canine subjects were scored by the (blinded) study veterinarian on days 0 and 30 using a scale of 1 (best) to 5 (worst) for four different movements consisting of sitting to standing, lying to standing, walking, and running. Data are represented as pie charts indicating percent of each cohort that showed improvement, worsening, or no change in condition for the animals enrolled in each study group. **p<0.01, ****p<0.001 by Pearson’s chi-squared.
Figure 7. Daily administration of CBD for 30 days does not alter alanine aminotransferase (ALT) or alkaline phosphatase (ALKP) levels.

Blood was drawn from animals we enrolled in the clinical study on days 0 and 30, and Chem10 analysis was performed. A. Relative changes in circulating ALT and ALKP values over the 30-day period. B. Specific changes in circulating ALT and ALKP values over the 30-day period. Dark horizontal lines outline normal range. Error bars +/− SD. No statistically significant changes were observed.
Table 2.
Veterinary Study CBC, Metabolic Panel, and Clinical Chemistry Values

|
Discussion
Arthritis is a painful degenerative condition that impacts the lives of almost a quarter of all Americans, with osteoarthritis in particular accounting for 60% of all-cause arthritis diagnoses. [2; 23] Because current treatment regimens are not curative and can be accompanied by significant co-morbidities [6; 9; 36], the present studies were undertaken to validate whether the recently-legalized supplement cannabidiol (CBD) might positively impact the symptomology of this degenerative condition. We first validated the widely-reported anti-inflammatory effects of CBD administration both in vitro and in vivo, demonstrating substantial impact upon inflammatory cytokines and innate immune cell subsets relevant to the pathophysiology of arthritis. Following additional experimentation that established greater bioavailability of liposomally-encapsulated vs. naked CBD in both mice and humans, we demonstrated the short-term clinical efficacy of CBD in a double-blind, placebo-controlled veterinary study in which neither owner nor veterinarian knew the content of the study medications. In this study, neither animals given placebo nor animals given a low daily dose of naked CBD responded to therapy in any significant fashion. Conversely, animals given a high dose of naked CBD or a low dose of liposomally-encapsulated CBD experienced significant improvements in quality of life scores as documented by both owner and veterinarian assessments. In this setting, administration of CBD was not associated with any significant alterations to circulating lymphocyte subsets, clinical chemistry values, or assessed metabolic parameters.
In vitro and in vivo studies focused on important pathologic mechanisms applicable to a wide variety of arthritis etiologies. We found that CBD significantly reduced LPS- and SEB-induced production of TNF-⍺ in human and mouse cell lines and PBMC, consistent with the results of previous studies. [3; 51; 60] Similarly, in a croton oil-induced murine model of inflammation, we found that topical administration of CBD significantly reduced TNF-⍺ production and MPO activity, the latter of which is consistent with previous reports of systemic CBD administration in mice. [4; 50] Consistent with previous in vivo studies, we demonstrated that CBD also significantly reduced LPS-induced pro-inflammatory cytokine [33; 37] and neutrophil production [40], while increasing anti-inflammatory IL-10 production in a dose-responsive fashion. [33] Given the wide variety of grades, formulations, and suppliers of commercially available CBD, it was important to validate and characterize the functional activity of the CBD isolate planned for use in subsequent veterinary studies. In those studies, the finding that 50 mg/day of naked CBD improved treatment outcomes is consistent with a previous study in dogs with OA [14]; however, this is the first report of a randomized, double-blind, placebo-controlled study that utilizes a spontaneous model for assessing the potential therapeutic effects of CBD for treating OA pain and increasing quality of life. As in humans, the pathogenesis of canine OA involves changes in all tissues of the synovial joint. [5; 24; 31; 34; 38] The dominant symptom of OA for both humans and dogs is pain, and the current therapeutic goal for both species is management of that pain and associated movement deficits. [7] Thus, an extrapolation of these findings suggest that CBD could be useful for treating pain and improving quality of life in humans with an affirmative diagnosis of osteoarthritis and/or other inflammatory conditions that might be ameliorated by a reduction in proinflammatory cytokines and pathologic neutrophil activity.
The absorption of CBD administered by smoking, vaporization, buccal spray, or oral ingestion is highly variable and results in extremely inconsistent pharmacokinetic (PK) profiles when investigated. [21; 39; 42; 44; 52] CBD also shows limited oral bioavailability due to poor aqueous solubility and extensive first-pass metabolism. [22; 41; 55] While the current study did not assess PK parameters among canine study participants, the effect of liposomal CBD on LPS-induced TNF-α production in mice provides an objective measure of its pharmacodynamic drug action and suggests a greater bioavailability than naked CBD. Although prior studies regarding the bioavailability of liposomal CBD are not found in the literature, a single study of Δ9-tetrahydrocannabinol (THC), the main psychoactive constituent in cannabis, reported that liposomal-encapsulation improved bioavailability in rats in comparison to administration of the naked molecule. [53] Based upon these animal studies, we performed an IRB-approved crossover study in healthy human volunteers to validate approved bioavailability of CBD following liposomal encapsulation. The data demonstrated a 17-fold increase in bioavailable circulating CBD following oral administration of the liposomal formulation as compared to the naked isolate.
Conclusions
In summary, we demonstrate here that the widely-available supplement cannabidiol (CBD) exerts robust and quantifiable anti-inflammatory properties in experimental systems. These experimental results were translatable in a randomized, double-blind, placebo controlled trial in a spontaneous canine model of osteoarthritis. In this assessment, administration of liposomally-encapsulated or high-dose naked CBD (but not low-dose naked CBD or placebo) was associated with significant improvements to quality of life as quantitated by both owner and veterinarian. The results suggest that clinical studies in humans may be warranted in a variety of different etiologies and disease stages of arthritis.
Supplementary Material
Table S1. Basic Characteristics of Enrolled Canine Subjects
Acknowledgements
This study was funded in part by a sponsored research agreement (to MMH) between Medterra CBD, Inc and Baylor College of Medicine. This project was also supported in part by the Cytometry and Cell Sorting Core at Baylor College of Medicine with funding from the NIH (AI036211, CA125123, and RR024574). Flow cytometry analysis was performed with the expert assistance of Joel M. Sederstrom.
Non-Standard Abbreviations
- ALKP
Alkaline phosphatase
- ALT
Alanine aminotransferase
- ANOVA
Analysis of variance
- APC
Allophycocyanin
- BSA
Bovine serum albumin
- CBC
Complete blood count
- CBD
Cannabidiol
- CD
Cluster of differentiation
- CXCL
C-X-C motif ligand
- Cy7
Cyanine 7
- DMARD
Disease modifying antirheumatic drug
- ECS
Endocannabinoid system
- EDTA
Ethylenediaminetetraacetic acid
- ELISA
Enzyme-linked immunoabsorbent assay
- ES
Effect size
- FITC
Fluorescein isothiocyanate
- HCPI
Helsinki chronic pain index
- HPLC
High performance liquid chromatography
- IACUC
Institutional animal care and use committee
- IL
Interleukin
- IRB
Institutional review board
- IVIS
In vivo imaging system
- Kras
Kirsten Rat Sarcoma (virus)
- LOQ
Limit of quantification
- LPS
Lipopolysaccharide
- Ly6G
Lymphocyte antigen 6 complex, locus G
- MPO
Myeloperoxidase
- NSAID
Nonsteroidal anti-inflammatory
- OA
Osteoarthritis
- OD
Optical density
- PBMC
Peripheral blood mononuclear cells
- PE
Phycoerythrin
- PK
Pharmacokinetic
- QOL
Quality of life
- SD
Standard deviation
- SEB
Staphylococcal enterotoxin B
- TEM
Transmission electron microscopy
- THC
Tetrahydrocannabinol
- TMB
Tetramethylbenzidine
- TNF
Tumor necrosis factor
Footnotes
Declaration of interests
Institutional policy requires WKD, MMH, and VK to declare their ownership stakes in Diakonos Research, Ltd, an unrelated immuno-oncology company. Additionally, MMH is a paid scientific advisor for Medterra CBD. All other authors declare no competing interests.
References
- [1].Bannwarth B Acetaminophen or NSAIDs for the treatment of osteoarthritis. Best Pract Res Clin Rheumatol 2006;20(1):117–129. [DOI] [PubMed] [Google Scholar]
- [2].Barbour KE, Helmick CG, Boring M, Brady TJ. Vital Signs: Prevalence of Doctor-Diagnosed Arthritis and Arthritis-Attributable Activity Limitation - United States, 2013–2015. MMWR Morb Mortal Wkly Rep 2017;66(9):246–253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Ben-Shabat S, Hanus LO, Katzavian G, Gallily R. New cannabidiol derivatives: synthesis, binding to cannabinoid receptor, and evaluation of their antiinflammatory activity. J Med Chem 2006;49(3):1113–1117. [DOI] [PubMed] [Google Scholar]
- [4].Borrelli F, Aviello G, Romano B, Orlando P, Capasso R, Maiello F, Guadagno F, Petrosino S, Capasso F, Di Marzo V, Izzo AA. Cannabidiol, a safe and non-psychotropic ingredient of the marijuana plant Cannabis sativa, is protective in a murine model of colitis. J Mol Med (Berl) 2009;87(11):1111–1121. [DOI] [PubMed] [Google Scholar]
- [5].Brandt KD, Braunstein EM, Visco DM, O’Connor B, Heck D, Albrecht M. Anterior (cranial) cruciate ligament transection in the dog: a bona fide model of osteoarthritis, not merely of cartilage injury and repair. J Rheumatol 1991;18(3):436–446. [PubMed] [Google Scholar]
- [6].Bullock J, Rizvi SAA, Saleh AM, Ahmed SS, Do DP, Ansari RA, Ahmed J. Rheumatoid Arthritis: A Brief Overview of the Treatment. Med Princ Pract 2018;27(6):501–507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Cimino Brown D What can we learn from osteoarthritis pain in companion animals? Clin Exp Rheumatol 2017;35 Suppl 107(5):53–58. [PubMed] [Google Scholar]
- [8].Clayton N, Collins S, Sargent R, Brown T, Nobbs M, Bountra C, Trezise D. The effect of the novel sodium channel blocker 4030W92 in models of acute and chronic inflammatory pain in the rat. British journal of pharmacology 1998;123. [Google Scholar]
- [9].Cooper C, Bardin T, Brandi ML, Cacoub P, Caminis J, Civitelli R, Cutolo M, Dere W, Devogelaer JP, Diez-Perez A, Einhorn TA, Emonts P, Ethgen O, Kanis JA, Kaufman JM, Kvien TK, Lems WF, McCloskey E, Miossec P, Reiter S, Ringe J, Rizzoli R, Saag K, Reginster JY. Balancing benefits and risks of glucocorticoids in rheumatic diseases and other inflammatory joint disorders: new insights from emerging data. An expert consensus paper from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Aging Clin Exp Res 2016;28(1):1–16. [DOI] [PubMed] [Google Scholar]
- [10].Couch DG, Cook H, Ortori C, Barrett D, Lund JN, O’Sullivan SE. Palmitoylethanolamide and Cannabidiol Prevent Inflammation-induced Hyperpermeability of the Human Gut In Vitro and In Vivo-A Randomized, Placebo-controlled, Double-blind Controlled Trial. Inflamm Bowel Dis 2019;25(6):1006–1018. [DOI] [PubMed] [Google Scholar]
- [11].Couch DG, Tasker C, Theophilidou E, Lund JN, O’Sullivan SE. Cannabidiol and palmitoylethanolamide are anti-inflammatory in the acutely inflamed human colon. Clin Sci (Lond) 2017;131(21):2611–2626. [DOI] [PubMed] [Google Scholar]
- [12].del Rio C, Navarrete C, Collado JA, Bellido ML, Gomez-Canas M, Pazos MR, Fernandez-Ruiz J, Pollastro F, Appendino G, Calzado MA, Cantarero I, Munoz E. The cannabinoid quinol VCE-004.8 alleviates bleomycin-induced scleroderma and exerts potent antifibrotic effects through peroxisome proliferator-activated receptor-gamma and CB2 pathways. Sci Rep 2016;6:21703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Gallily R, Yekhtin Z, Hanus LO. The Anti-Inflammatory Properties of Terpenoids from Cannabis. Cannabis Cannabinoid Res 2018;3(1):282–290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Gamble LJ, Boesch JM, Frye CW, Schwark WS, Mann S, Wolfe L, Brown H, Berthelsen ES, Wakshlag JJ. Pharmacokinetics, Safety, and Clinical Efficacy of Cannabidiol Treatment in Osteoarthritic Dogs. Front Vet Sci 2018;5:165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Hammell DC, Zhang LP, Ma F, Abshire SM, McIlwrath SL, Stinchcomb AL, Westlund KN. Transdermal cannabidiol reduces inflammation and pain-related behaviours in a rat model of arthritis. Eur J Pain 2016;20(6):936–948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Haraden CA, Huebner JL, Hsueh MF, Li YJ, Kraus VB. Synovial fluid biomarkers associated with osteoarthritis severity reflect macrophage and neutrophil related inflammation. Arthritis Res Ther 2019;21(1):146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Hay M, Thomas DW, Craighead JL, Economides C, Rosenthal J. Clinical development success rates for investigational drugs. Nature biotechnology 2014;32(1):40–51. [DOI] [PubMed] [Google Scholar]
- [18].Hielm-Bjorkman AK, Rita H, Tulamo RM. Psychometric testing of the Helsinki chronic pain index by completion of a questionnaire in Finnish by owners of dogs with chronic signs of pain caused by osteoarthritis. Am J Vet Res 2009;70(6):727–734. [DOI] [PubMed] [Google Scholar]
- [19].Hill R NK1 (substance P) receptor antagonists--why are they not analgesic in humans? Trends Pharmacol Sci 2000;21(7):244–246. [DOI] [PubMed] [Google Scholar]
- [20].Huang Y, Wan T, Pang N, Zhou Y, Jiang X, Li B, Gu Y, Huang Y, Ye X, Lian H, Zhang Z, Yang L. Cannabidiol protects livers against nonalcoholic steatohepatitis induced by high-fat high cholesterol diet via regulating NF-kappaB and NLRP3 inflammasome pathway. J Cell Physiol 2019;234(11):21224–21234. [DOI] [PubMed] [Google Scholar]
- [21].Huestis MA. Pharmacokinetics and metabolism of the plant cannabinoids, delta9-tetrahydrocannabinol, cannabidiol and cannabinol. Handb Exp Pharmacol 2005(168):657–690. [DOI] [PubMed] [Google Scholar]
- [22].Huestis MA. Human cannabinoid pharmacokinetics. Chem Biodivers 2007;4(8):1770–1804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet 2019;393(10182):1745–1759. [DOI] [PubMed] [Google Scholar]
- [24].Innes JF, Fuller CJ, Grover ER, Kelly AL, Burn JF. Randomised, double-blind, placebo-controlled parallel group study of P54FP for the treatment of dogs with osteoarthritis. Vet Rec 2003;152(15):457–460. [DOI] [PubMed] [Google Scholar]
- [25].Jastrzab A, Gegotek A, Skrzydlewska E. Cannabidiol Regulates the Expression of Keratinocyte Proteins Involved in the Inflammation Process through Transcriptional Regulation. Cells 2019;8(8). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Kapoor M, Martel-Pelletier J, Lajeunesse D, Pelletier JP, Fahmi H. Role of proinflammatory cytokines in the pathophysiology of osteoarthritis. Nat Rev Rheumatol 2011;7(1):33–42. [DOI] [PubMed] [Google Scholar]
- [27].Katchan V, David P, Shoenfeld Y. Cannabinoids and autoimmune diseases: A systematic review. Autoimmun Rev 2016;15(6):513–528. [DOI] [PubMed] [Google Scholar]
- [28].Kawase Y, Hoshino T, Yokota K, Kuzuhara A, Kirii Y, Nishiwaki E, Maeda Y, Takeda J, Okamoto M, Kato S, Imaizumi T, Aizawa H, Yoshino K. Exacerbated and prolonged allergic and non-allergic inflammatory cutaneous reaction in mice with targeted interleukin-18 expression in the skin. J Invest Dermatol 2003;121(3):502–509. [DOI] [PubMed] [Google Scholar]
- [29].Kolhekar R, Meller ST, Gebhart GF. N-methyl-D-aspartate receptor-mediated changes in thermal nociception: allosteric modulation at glycine and polyamine recognition sites. Neuroscience 1994;63(4):925–936. [DOI] [PubMed] [Google Scholar]
- [30].Krajewska JB, Bartoszek A, Fichna J. New Trends in Liposome-based Drug Delivery in Colorectal Cancer. Mini Rev Med Chem 2019;19(1):3–11. [DOI] [PubMed] [Google Scholar]
- [31].Lang J, Busato A, Baumgartner D, Fluckiger M, Weber UT. Comparison of two classification protocols in the evaluation of elbow dysplasia in the dog. J Small Anim Pract 1998;39(4):169–174. [DOI] [PubMed] [Google Scholar]
- [32].Lin J, Zhang W, Jones A, Doherty M. Efficacy of topical non-steroidal anti-inflammatory drugs in the treatment of osteoarthritis: meta-analysis of randomised controlled trials. BMJ 2004;329(7461):324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Liu DZ, Hu CM, Huang CH, Wey SP, Jan TR. Cannabidiol attenuates delayed-type hypersensitivity reactions via suppressing T-cell and macrophage reactivity. Acta Pharmacol Sin 2010;31(12):1611–1617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Liu W, Burton-Wurster N, Glant TT, Tashman S, Sumner DR, Kamath RV, Lust G, Kimura JH, Cs-Szabo G. Spontaneous and experimental osteoarthritis in dog: similarities and differences in proteoglycan levels. J Orthop Res 2003;21(4):730–737. [DOI] [PubMed] [Google Scholar]
- [35].Lowin T, Schneider M, Pongratz G. Joints for joints: cannabinoids in the treatment of rheumatoid arthritis. Curr Opin Rheumatol 2019;31(3):271–278. [DOI] [PubMed] [Google Scholar]
- [36].Luis M, Freitas J, Costa F, Buttgereit F, Boers M, Jap DS, Santiago T. An updated review of glucocorticoid-related adverse events in patients with rheumatoid arthritis. Expert Opin Drug Saf 2019;18(7):581–590. [DOI] [PubMed] [Google Scholar]
- [37].Malfait AM, Gallily R, Sumariwalla PF, Malik AS, Andreakos E, Mechoulam R, Feldmann M. The nonpsychoactive cannabis constituent cannabidiol is an oral anti-arthritic therapeutic in murine collagen-induced arthritis. Proc Natl Acad Sci U S A 2000;97(17):9561–9566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].McCoy AM. Animal Models of Osteoarthritis: Comparisons and Key Considerations. Vet Pathol 2015;52(5):803–818. [DOI] [PubMed] [Google Scholar]
- [39].McGilveray IJ. Pharmacokinetics of cannabinoids. Pain Res Manag 2005;10 Suppl A:15A–22A. [DOI] [PubMed] [Google Scholar]
- [40].McHugh D, Tanner C, Mechoulam R, Pertwee RG, Ross RA. Inhibition of human neutrophil chemotaxis by endogenous cannabinoids and phytocannabinoids: evidence for a site distinct from CB1 and CB2. Mol Pharmacol 2008;73(2):441–450. [DOI] [PubMed] [Google Scholar]
- [41].Mechoulam R, Parker LA, Gallily R. Cannabidiol: an overview of some pharmacological aspects. J Clin Pharmacol 2002;42(S1):11S–19S. [DOI] [PubMed] [Google Scholar]
- [42].Millar SA, Stone NL, Yates AS, O’Sullivan SE. A Systematic Review on the Pharmacokinetics of Cannabidiol in Humans. Front Pharmacol 2018;9:1365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Muthumalage T, Rahman I. Cannabidiol differentially regulates basal and LPS-induced inflammatory responses in macrophages, lung epithelial cells, and fibroblasts. Toxicol Appl Pharmacol 2019;382:114713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Ohlsson A, Lindgren JE, Andersson S, Agurell S, Gillespie H, Hollister LE. Single-dose kinetics of deuterium-labelled cannabidiol in man after smoking and intravenous administration. Biomed Environ Mass Spectrom 1986;13(2):77–83. [DOI] [PubMed] [Google Scholar]
- [45].Orange DE, Blachere NE, DiCarlo EF, Mirza S, Pannellini T, Jiang CS, Frank MO, Parveen S, Figgie MP, Gravallese EM, Bykerk VP, Orbai AM, Mackie SL, Goodman SM. Rheumatoid arthritis morning stiffness is associated with synovial fibrin and neutrophils. Arthritis Rheumatol 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Park J, Mendy A, Vieira ER. Various Types of Arthritis in the United States: Prevalence and Age-Related Trends From 1999 to 2014. Am J Public Health 2018;108(2):256–258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Petrosino S, Verde R, Vaia M, Allara M, Iuvone T, Di Marzo V. Anti-inflammatory Properties of Cannabidiol, a Nonpsychotropic Cannabinoid, in Experimental Allergic Contact Dermatitis. J Pharmacol Exp Ther 2018;365(3):652–663. [DOI] [PubMed] [Google Scholar]
- [48].Philpott HT, O’Brien M, McDougall JJ. Attenuation of early phase inflammation by cannabidiol prevents pain and nerve damage in rat osteoarthritis. Pain 2017;158(12):2442–2451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [49].Ridgley LA, Anderson AE, Pratt AG. What are the dominant cytokines in early rheumatoid arthritis? Curr Opin Rheumatol 2018;30(2):207–214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].Schicho R, Storr M. Topical and systemic cannabidiol improves trinitrobenzene sulfonic acid colitis in mice. Pharmacology 2012;89(3–4):149–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [51].Silva RL, Silveira GT, Wanderlei CW, Cecilio NT, Maganin AGM, Franchin M, Marques LMM, Lopes NP, Crippa JA, Guimaraes FS, Alves-Filho JCF, Cunha FQ, Cunha TM. DMH-CBD, a cannabidiol analog with reduced cytotoxicity, inhibits TNF production by targeting NF-kB activity dependent on A2A receptor. Toxicol Appl Pharmacol 2019;368:63–71. [DOI] [PubMed] [Google Scholar]
- [52].Stott CG, White L, Wright S, Wilbraham D, Guy GW. A phase I study to assess the effect of food on the single dose bioavailability of the THC/CBD oromucosal spray. Eur J Clin Pharmacol 2013;69(4):825–834. [DOI] [PubMed] [Google Scholar]
- [53].Szczesniak AM, Kelly ME, Whynot S, Shek PN, Hung O. Ocular hypotensive effects of an intratracheally delivered liposomal delta9-tetrahydrocannabinol preparation in rats. J Ocul Pharmacol Ther 2006;22(3):160–167. [DOI] [PubMed] [Google Scholar]
- [54].Towheed TE, Maxwell L, Judd MG, Catton M, Hochberg MC, Wells G. Acetaminophen for osteoarthritis. Cochrane Database Syst Rev 2006(1):CD004257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [55].Ujvary I, Hanus L. Human Metabolites of Cannabidiol: A Review on Their Formation, Biological Activity, and Relevance in Therapy. Cannabis Cannabinoid Res 2016;1(1):90–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [56].Vincent TL, Williams RO, Maciewicz R, Silman A, Garside P, Arthritis Research UKamwg. Mapping pathogenesis of arthritis through small animal models. Rheumatology (Oxford) 2012;51(11):1931–1941. [DOI] [PubMed] [Google Scholar]
- [57].Vuolo F, Abreu SC, Michels M, Xisto DG, Blanco NG, Hallak JE, Zuardi AW, Crippa JA, Reis C, Bahl M, Pizzichinni E, Maurici R, Pizzichinni MMM, Rocco PRM, Dal-Pizzol F. Cannabidiol reduces airway inflammation and fibrosis in experimental allergic asthma. Eur J Pharmacol 2019;843:251–259. [DOI] [PubMed] [Google Scholar]
- [58].Wallace MS, Rowbotham M, Bennett GJ, Jensen TS, Pladna R, Quessy S. A multicenter, double-blind, randomized, placebo-controlled crossover evaluation of a short course of 4030W92 in patients with chronic neuropathic pain. The journal of pain : official journal of the American Pain Society 2002;3(3):227–233. [DOI] [PubMed] [Google Scholar]
- [59].Wallace MS, Rowbotham MC, Katz NP, Dworkin RH, Dotson RM, Galer BS, Rauck RL, Backonja MM, Quessy SN, Meisner PD. A randomized, double-blind, placebo-controlled trial of a glycine antagonist in neuropathic pain. Neurology 2002;59(11):1694–1700. [DOI] [PubMed] [Google Scholar]
- [60].Watzl B, Scuderi P, Watson RR. Influence of marijuana components (THC and CBD) on human mononuclear cell cytokine secretion in vitro. Adv Exp Med Biol 1991;288:63–70. [DOI] [PubMed] [Google Scholar]
- [61].Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, Bierma-Zeinstra S, Brandt KD, Croft P, Doherty M, Dougados M, Hochberg M, Hunter DJ, Kwoh K, Lohmander LS, Tugwell P. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage 2008;16(2):137–162. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Basic Characteristics of Enrolled Canine Subjects