
Fig. 1.
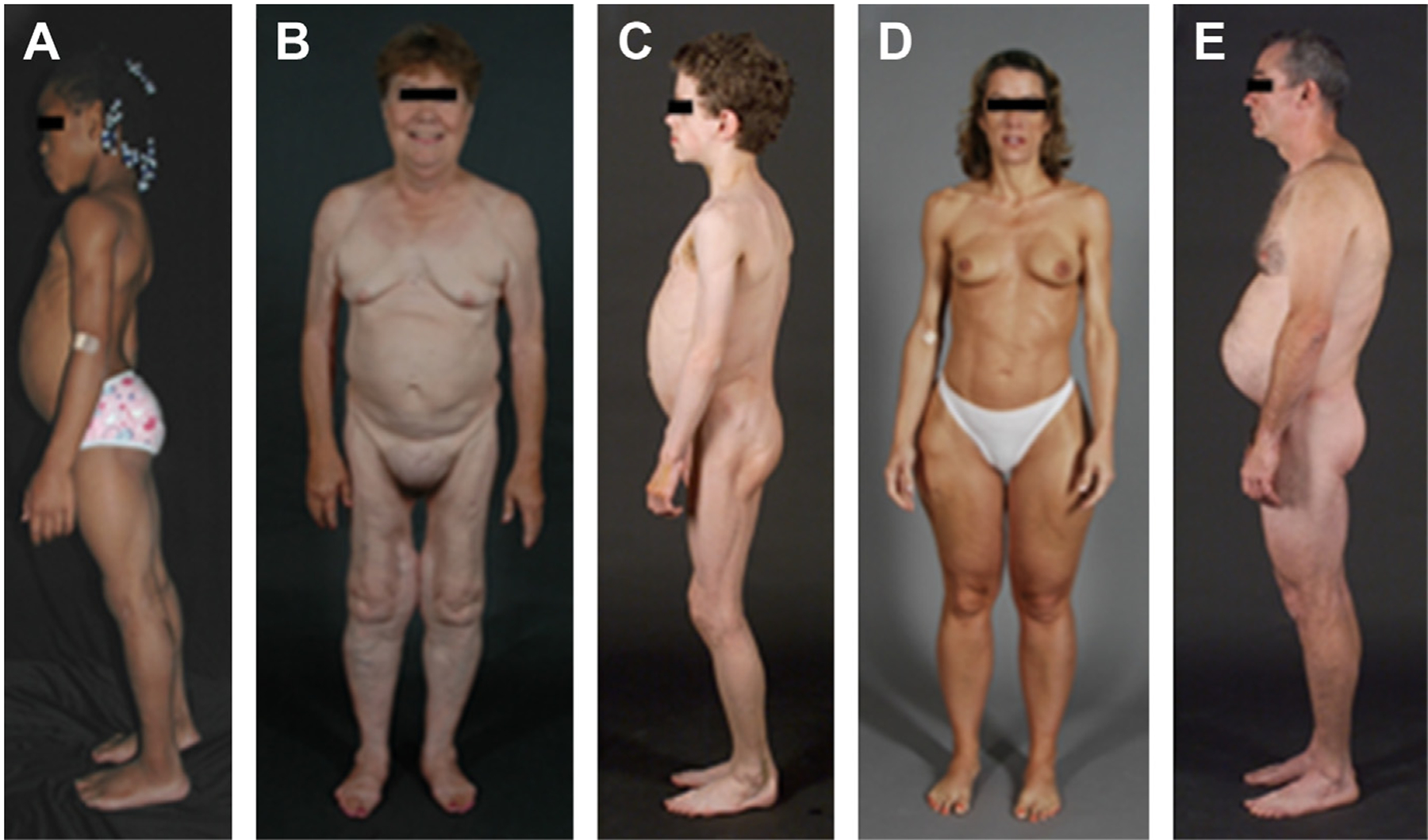
Clinical features of patients with various types of lipodystrophies. (A) Lateral view of an 8-year-old African American girl with congenital generalized lipodystrophy (also known as Berardinelli-Seip congenital lipodystrophy) type 1 caused by homozygous c.377insT (p.Leu126fs*146) mutation in AGPAT2. The patient had generalized loss of subcutaneous fat at birth and developed mild acanthosis nigricans in the axillae and neck later during childhood. She had umbilical prominence and acromegaloid features (enlarged mandible, hands, and feet). (B) Anterior view of a 65-year-old white woman with familial partial lipodystrophy of the Dunnigan variety caused by heterozygous p.Arg482Gln mutation in LMNA. She noticed loss of subcutaneous fat from the limbs at the time of puberty and later lost subcutaneous fat from the anterior truncal region. The breasts were atrophic. She had increased subcutaneous fat deposits in the face, anterior neck, suprapubic and vulvar region, and medial parts of the knees. (C) Lateral view of an 8-year-old German boy with acquired generalized lipodystrophy. He started experiencing generalized loss of subcutaneous fat at age 3 with marked acanthosis nigricans in the neck, axillae, and groin. He developed Crohn’s disease at age 11 requiring hemicolectomy at age 13. (D) Anterior view of a 39-year-old white woman with acquired partial lipodystrophy (Barraquer-Simons syndrome). She noticed marked loss of subcutaneous fat from the face, neck, upper extremities, chest, and abdomen at the age of 12 years but later developed increased subcutaneous fat deposition in the lower extremities. (E) Lateral view of a 39-year-old white man infected with HIV with protease inhibitor–containing highly active antiretroviral therapy–induced lipodystrophy. He had marked loss of subcutaneous fat from the face and limbs but had increased subcutaneous fat deposition in the neck region anteriorly and posteriorly showing buffalo hump. Abdomen was protuberant because of excess intra-abdominal fat. He had been on protease inhibitor–containing antiretroviral therapy for more than 7 years. ([A] From Simha V, Garg A. Lipodystrophy: lessons in lipid and energy metabolism. Curr Opin Lipidol 2006;17:162–9; with permission; [B–E] Garg A. Lipodystrophies: genetic and acquired body fat disorders. J Clin Endocrinol Metab 2011;96:3317; with permission.)