

Abstract
Background:
Physician burnout has been a global problem that affects severely the mental status among doctors, especially in emergency medicine (EM). However, few studies have focused on emergency medicine physicians, and the published data are inconsistent. Thus, this meta-analysis is performed to systematically evaluate the prevalence of burnout among emergency medicine physicians.
Methods:
We systematically searched databases including PubMed, Embase, PsychINFO and the Cochrane Library from inception to September, 2019 for English-language articles. We selected all the original articles those used Maslach Burnout Inventory to assess the prevalence of burnout and its 3 dimensions emotional exhaustion (EE), depersonalization, and personal accomplishment (PA) in emergency medicine physicians. After literature screening, quality evaluation was performed for eligible studies by using the Joanna Briggs Institute (JBI) critical appraisal checklist for studies reporting prevalence data; then, Begg test and Egger test was used to assess publication bias. Pooled prevalence rates were assessed by conducting a meta-analysis using random effects models. Then sensitivity analysis followed to test the stability of the result and detected the source of heterogeneity.
Results:
A total of 1943 EM physicians provided burnout data. The pooled prevalence rates of high levels of emotional exhaustion, high levels of depersonalization and low levels of PA were 40% (95% CI: 26%–55%; I2 = 97.4%), 41% (95% CI: 30%–52%; I2 = 94.5%) and 35% (95% CI: 19%–52%; I2 = 99.0%), respectively. The mean burnout scores were 23.95 (SD = 11.88) for emotional exhaustion, 11.63 (SD = 6.85) for depersonalization, and 34.69 (SD = 7.71) for PA.
Conclusions:
This meta-analysis demonstrate a high level of burnout prevalent in EM physicians that approximately 40% experience high levels of EE and depersonalization. Our findings also suggest that EM physicians are more susceptible to burnout compared with physicians in other departments and other medical staffs in EM. More attention should be payed to mental status of EM physicians and further investigation concerning how to reduce burnout would be beneficial for EM physicians.
Registration: INPLASY202060060 in inplasy.com (doi.org/10.37766/inplasy2020.6.0060)
Keywords: burnout, emergency medicine, Maslach Burnout Inventory, physicians
1. Introduction
Sudden deaths resulting from heavy workloads among physicians sharply increased from 2008 to 2015 in China.[1] In fact, physician burnout is also a serious issue at the global level.[2] Physician burnout not only negatively impacts the health of physicians but also has been associated with a higher risk of adversely influencing patient outcomes (odds ratio 1.96, 95% CI 1.59–2.40).[3,4]
Burnout is the most common chronic work-related stress exposure, and it has an especially high occurrence rate in emergency medicine (EM) physicians.[5,6] It has been reported that the prevalence of burnout is higher than 60% among EM physicians when assessed using the Maslach Burnout Inventory (MBI).[7] Compared with physicians in other departments (38%) and the general population (30%), EM physicians are particularly susceptible to burnout.[8] Considering the challenging and stressful nature of EM, the potential adverse consequences underscore the importance of understanding burnout among EM physicians.[9]
Some research concerning burnout among EM staff has been conducted.[10,11] However, few studies have focused on EM physicians, and the published data are inconsistent. Thus, we performed a meta-analysis to systematically evaluate the prevalence of burnout among EM physicians. To the best of our knowledge, this is the first meta-analysis focusing on all 3 subscales of burnout measured by the MBI scales among EM physicians.
2. Methods
2.1. Registration and ethical approval
The systematic review and meta-analysis was conducted following an established protocol (INPLASY202060060).[12] Our study is based on published data; thus, ethical approval is not a requirement.
2.2. Search strategy
This meta-analysis was performed according to the PRISMA statement.[13] To identify relevant studies, we searched PubMed (prior to September 7, 2019), Embase (Ovid; 1974 to September 6, 2019), PsychINFO (Ovid; 1806 to September 1, 2019) and the Cochrane Library (Ovid; prior to September 5, 2019). The detailed search terms are shown in the supplementary materials. We also checked the references of the relevant literature.
2.3. Eligibility criteria
The PICOS-guided eligible criteria included the following:
-
1)
Population (P): participants were EM physicians suffering from burnout
-
2)
Studies that used MBI to assess burnout with sufficient data
-
3)
Outcomes (O): the prevalence of burnout and its 3 dimensions; and
-
4)
Study design (S): cross-section studies and intervention studies. We excluded the following literature: conference abstracts, reviews, letters, case reports, unpublished data, and insufficient data. The eligibility assessment was performed by 2 investigators, and disagreements were resolved by discussion among all the authors.
2.4. Data extraction
Extraction was conducted by 2 investigators independently. The following information was extracted: study characteristics (first author, publication year, country, number of participants, response rate), participant characteristics (mean age, sex ratio), and outcome-related data [prevalence rates of high levels of emotional exhaustion (EE > 26), high levels of depersonalization (DP >9) and low levels of personal accomplishment (PA < 34)]. Mean scores calculated by the Maslach Burnout Inventory-Health Services Survey (MBI-HSS) were collected.
2.5. Evaluation of study quality
The Joanna Briggs Institute's (JBI) critical appraisal checklist for studies reporting prevalence data was utilized to evaluate the quality of the studies. This tool assessed studies according to 9 questions. If the answer was yes, the question was assigned a score of 1. If the answer was no, unclear or not applicable, it was assigned a score of 0. Total quality scores ≤ 4, 5 to 7 and ≥ 8 were regarded as low, moderate, and high quality, respectively. The evaluation of study quality was performed by 2 investigators, and disagreements were settled by discussion.
2.6. Statistical analysis
The aggregate prevalence of EE, DP and PA were pooled using STATA 12.0 software (STATA Corporation, College Station, TX). The between-study heterogeneities were assessed, with P < .10 or I2>50% indicating significant heterogeneity. If significant heterogeneity existed, the fixed effects model was used for the meta-analysis. If not, a random effects model was used, and the reasons for the heterogeneity were explored. In addition, sensitivity analyses were conducted to test the stability of the pooled prevalence by excluding studies one by one. Publication bias was assessed by Begg and Egger tests. If P > .05, there was no potential publication bias. Microsoft Excel 2013 was used to calculate the mean and standard deviation. The STATA codes and the detailed calculations are shown in the supplementary materials.
3. Results
3.1. Literature search
A total of 243 studies were identified, and no additional records were obtained from other sources. Among these 243 studies, 88 duplicated articles were removed. According to the inclusion and exclusion criteria, 62 records were excluded after screening the titles and abstracts. The full-text articles of the remaining records were assessed for eligibility, and 76 were removed due to a lack of physician-specific data (n = 39) or a lack of sufficient data (n = 4); in addition, reference abstracts (n = 23) and reviews (n = 10) were excluded. Finally, 17 articles were included in our analysis. The process of screening and selecting studies for inclusion is shown in Figure 1.
Figure 1.
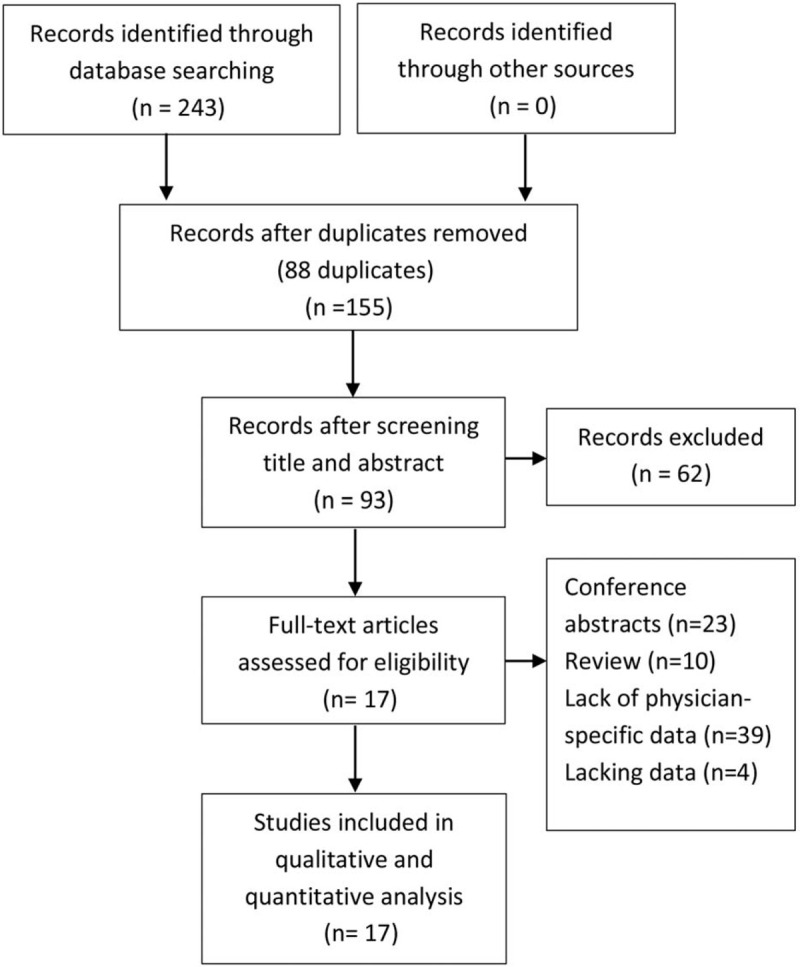
Flow diagram.
3.2. Study characteristics
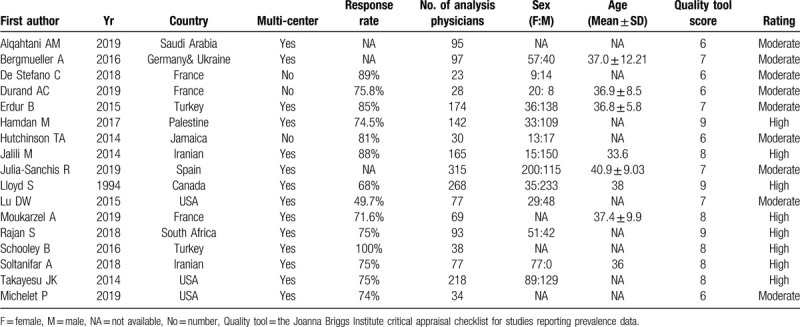
A total of 17 studies across 12 different countries and involving 1943 EM physicians were included. The mean ages of these participants were approximately 35 to 40 years old. Sixteen studies were cross-sectional in design, and only 1 provided an intervention.[14] The participants in 14 studies were recruited from multiple centers, and the participants in 3 studies were recruited from a single center. The studies were appraised using the JBI quality assessment, and we rated 8 studies as high quality and 9 studies as medium quality; none of the studies were rated as low quality. The detailed baseline characteristics and quality assessment of the eligible studies are shown in Table 1.[14–30]
Table 1.
Characteristics of included studies.
3.3. Outcome analyses
Thirteen studies (1255 participants) reported prevalence rates of high levels on all 3 subscales of MBI (EE > 26, DP > 9, and low PA < 34), and 7 studies (1126 participants) provided a mean burnout score on the MBI-HSS. Due to the significant between-study heterogeneities (I2 > 50%), random effect models were used. Among 1255 EM physicians, the pooled prevalence rates of high levels of burnout on the EE, DP, and PA scales were 40% (95% CI: 26%–55%; I2 = 97.4%) (Fig. 2), 41% (95% CI: 30%–52%; I2 = 94.5%) (Fig. 3), and 35% (95% CI: 19%–52%; I2 = 99.0%) (Fig. 4), respectively. Of 1126 participants, the mean burnout scores were 23.95 for EE (SD = 11.88; moderate), 11.63 for DP (SD = 6.85; high), and 34.69 for PA (SD = 7.71; moderate).
Figure 2.
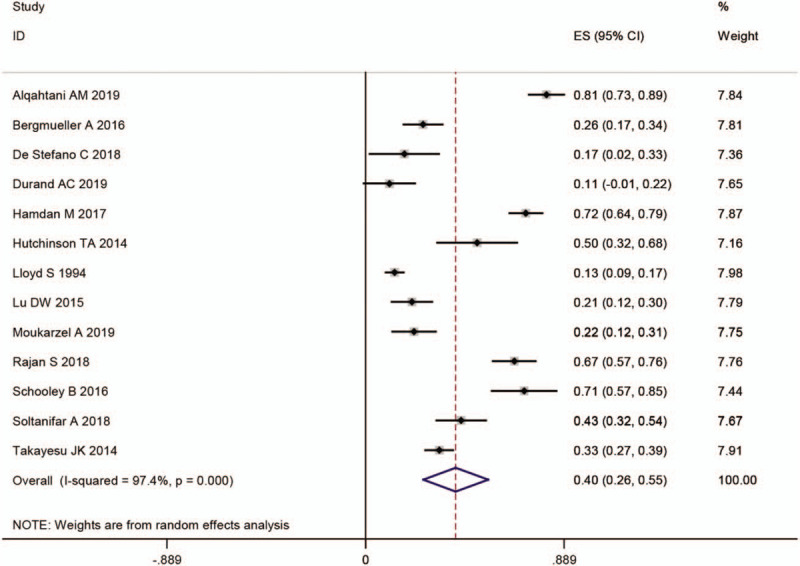
Prevalence of high levels of emotional exhaustion. CI = confidence interval, ES = prevalence.
Figure 3.
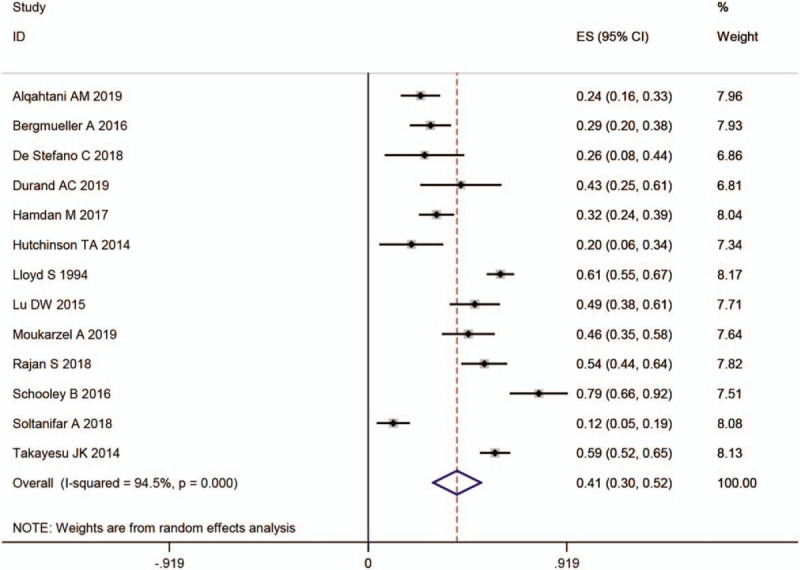
Prevalence of high levels of depersonalisation. CI = confidence interval, ES = prevalence.
Figure 4.
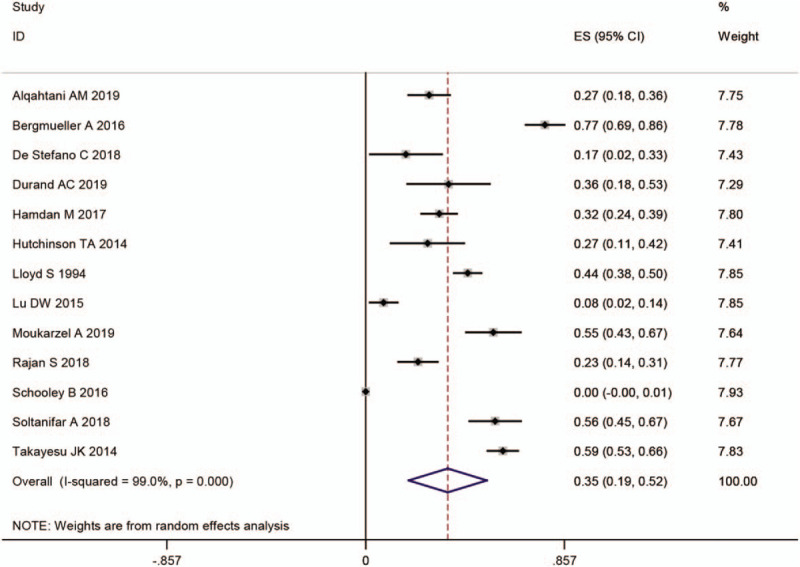
Prevalence of low personal accomplishment. CI = confidence interval, ES = prevalence.
3.4. Publication bias
Begg and Egger tests demonstrated no evidence of significant publication bias among the 13 studies that reported the prevalence of high levels of burnout (Fig. 5).
Figure 5.

Begg funnel plot of high levels of emotional exhaustion (A), high levels of depersonalization (B) and low levels of personal accomplishment (C).
3.5. Sensitivity analysis
Each study was removed one by one to test the stability of the pooled prevalence of all 3 subscales of MBI in the sensitivity analysis. The pooled prevalence of high levels of EE ranged from 37% (95% CI: 24%–50%; I2 = 96.4%) to 43% (95% CI: 28%–58%; I2 = 97.5%). The range was from 38.1% (95% CI: 27.2%–49%; I2 = 94.1%) to 43.8% (95% CI: 33.9%–53.7%; I2 = 92%) for the prevalence of high levels of DP and from 31.9% (95% CI: 16.2%–47.6%; I2 = 98.7%) to 38.5% (95% CI: 25.8%–51.3%; I2 = 96%) for the prevalence of low levels of PA. Hence, there was no obvious influence on the final results with the exclusion of any single study, which showed that our results are reliable.
4. Discussion
The department of EM is known for its emotional and physical challenges. Previous studies demonstrated that EM physicians experience higher than average levels of burnout, which leads to negative outcomes for patients as well as the physicians themselves.[8] However, the prevalence of burnout among EM physicians has not been well enough described to make people pay attention to this issue. This study was performed to evaluate the prevalence of burnout among EM physicians. A meta-analysis was performed to comprehensively understand burnout among EM physicians, and 13 studies were included. Our pooled analysis of the data demonstrated that approximately 40% of EM physicians experience high levels of EE and DP when assessed by MBI.
MBI, considered the gold standard tool for the measurement of physician burnout, involves EE, DP, and PA.[31] In the 3 subscale scores (EE, DP, low PA), higher levels of EE caused higher levels of DP, and both could successfully differentiate between burnout and non-burnout workers. Hence, researchers propose that high EE and high DP alone are vital components of burnout.[32] In our study, the prevalence of high levels of EE and DP were consistent, which supported the stability of the results.
Compared with medical staff in other professional categories, previous studies demonstrated that EM physicians were more susceptible to burnout, which also supports our findings. A meta-analysis pooling different professional physicians indicated that the prevalence of EE, DP and PA was 21% (95% CI 19–24, I2 = 94.7%), 29% (95% CI 25–33, I2 = 96.7%) and 29% (95% CI 24–34, I2 = 97.7%), respectively. Further analysis also found that EM physicians had significantly more severe burnout than other physicians (P = .019).[33] Similarly, another meta-analysis observed that oncology physicians had lower prevalence rates for high levels of EE, high levels of DP, and low levels of PA (32%, 24%, and 37%).[34] Furthermore, compared with other workers in the EM department, physicians is more prone to burnout. For example, a meta-analysis including 1566 emergency nurses observed that the prevalence of each subscale of MBI was 31% (95% CI, 20%–44%), 36% (95% CI, 23%–51%) and 29% (95% CI, 15%–44%) for high levels of EE, high levels of DP and low levels of PA, respectively.[35]
Several factors contribute to professional burnout. Working at night, working in the emergency department, experiencing job strain, experiencing a fear of making mistakes, experiencing sleep disorders, and experiencing workplace violence were the main factors significantly associated with higher burnout scores (P < .05) in the emergency department.[18,27] For individual factors, being younger, having fewer years of experience, being female, and having particular personality characteristics were most related to a high level of burnout.[16,30] Thus, effective measures focused on rest, recovery, and support might improve burnout.[24,28]
There are several limitations in this study. First, this meta-analysis included a limited number of studies. Therefore, more studies and a larger sample of participants are warranted to further clarify this issue. On the other hand, significant between-study heterogeneity is shown in our study whereas it is a common problem of meta-analyses for incidence rate. However, it was difficult to extract the factors associated with burnout for quantitative analysis. Further studies to analyze the related factors will provide useful information for healthcare professionals and policymakers to tackle EM physician burnout.
5. Conclusions
In conclusion, this meta-analysis demonstrates a high level of burnout prevalent in EM physicians that approximately 40% experience high levels of EE and DP. Our findings also suggest that EM physicians are more susceptible to burnout compared with physicians in other departments and other medical staffs in EM. More attention should be payed to mental status of EM physicians and further investigation concerning how to reduce burnout would be beneficial for EM physicians.
Acknowledgments
We are truly thankful to the editor's and reviewers’ constructive comments.
Author contributions
Conception and design: Zheng-chi Li and Qin Zhang.
Collection and assembly of data: Qin Zhang, Ming-chun Mu.
Data analysis and interpretation: Qin Zhang, Ming-chun Mu, Yan He, Zhao-lun Cai, Zheng-chi Li.
Manuscript writing and revising: Qin Zhang, Ming-chun Mu, Yan He, Zhao-lun Cai, Zheng-chi Li.
Final approval of manuscript: Qin Zhang, Ming-chun Mu, Yan He, Zhao-lun Cai, Zheng-chi Li.
Footnotes
Abbreviations: DP = depersonalization, EE = emotional exhaustion, EM = emergency medicine, MBI = Maslach Burnout Inventory, PA = personal accomplishment.
How to cite this article: Zhang Q, Mu M-c, He Y, Cai Z-l, Li Z-c. Burnout in emergency medicine physicians: a meta-analysis and systematic review. Medicine. 2020;99:32(e21462).
QZ and MM-c contributed equally to this work.
This work was supported by the Science and Technology Support Program of Sichuan Province (2019JDR0157).
The authors have no conflicts of interest to disclose.
The datasets generated during and/or analyzed during the current study are publicly available.
References
- [1].Song X-N, Shen J, Ling W, et al. Sudden deaths among Chinese physicians. Chinese Med J 2015;128:3251–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].The Lancet. Physician burnout: a global crisis. Lancet. 2019;394:93. [DOI] [PubMed] [Google Scholar]
- [3].Panagioti M, Geraghty K, Johnson J, et al. Association between physician burnout and patient safety, professionalism, and patient satisfaction: a systematic review and meta-analysis. JAMA Intern Med 2018;178:1317–30. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- [4].Yates SW. Physician stress and burnout. Am J Med 2020;133:160–4. [DOI] [PubMed] [Google Scholar]
- [5].Escriba-Aguir V, Perez-Hoyos S. Psychological well-being and psychosocial work environment characteristics among emergency medical and nursing staff. Stress Health 2007;23:153–60. [DOI] [PubMed] [Google Scholar]
- [6].Gulalp B, Karcioglu O, Sari A, et al. Burnout: need help? J Occup Med Toxicol 2008;3:32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med 2012;172:1377–85. [DOI] [PubMed] [Google Scholar]
- [8].Arora M, Asha S, Chinnappa J, et al. Review article: burnout in emergency medicine physicians emergency medicine Australasia. EMA 2013;25:491–5. [DOI] [PubMed] [Google Scholar]
- [9].Bragard I, Dupuis G, Fleet R. Quality of work life, burnout, and stress in emergency department physicians: a qualitative review. Eur J Emerg Med 2015;22:227–34. [DOI] [PubMed] [Google Scholar]
- [10].Lu DW, Weygandt PL, Pinchbeck C, et al. Emergency medicine trainee burnout is associated with lower patients’ satisfaction with their emergency department care. AEM Educ Train 2018;2:86–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Baier N, Roth K, Felgner S, et al. Burnout and safety outcomes - a cross-sectional nationwide survey of EMS-workers in Germany. BMC Emerg Med 2018;18:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Zhang et al. Burnout in emergency medicine physicians: a systematic review and meta-analysis. Inplasy Protoc 202060060. [Google Scholar]
- [13].Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol 2009;62:e1–34. [DOI] [PubMed] [Google Scholar]
- [14].Michelet P, Durand AC, Sebbane M, et al. Does implementation of a corporate wellness initiative improve burnout? Biomed Res Int 2019;20:138–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Alqahtani AM, Awadalla NJ, Alsaleem SA, et al. Burnout syndrome among emergency physicians and nurses in Abha and Khamis Mushait cities, Aseer region, Southwestern Saudi Arabia. SCI WORLD J 2019;2019:1–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Bergmueller A, Zavgorodnii I, Zavgorodnia N, et al. Relationship between burnout syndrome and personality characteristics in emergency ambulance crew. Neurosci Behav Physiol 2018;48:404–8. [Google Scholar]
- [17].De Stefano C, Philippon AL, Krastinova E, et al. Effect of emergency physician burnout on patient waiting times. Intem Emerg Med 2018;13:421–8. [DOI] [PubMed] [Google Scholar]
- [18].Durand AC, Bompard C, Sportiello J, et al. Stress and burnout among professionals working in the emergency department in a French University Hospital: prevalence and associated factors. Work 2019;63:57–67. [DOI] [PubMed] [Google Scholar]
- [19].Erdur B, Ergin A, Yuksel A, et al. Assessment of the relation of violence and burnout among physicians working in the emergency departments in Turkey. Ulus Travma Acil Cerrahi Derg 2015;21:175–81. [DOI] [PubMed] [Google Scholar]
- [20].Hamdan M, Hamra AAA. Burnout among workers in emergency departments in Palestinian hospitals: prevalence and associated factors. BMC Health Serv Res 2017;17:407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Hutchinson TA, Haase S, French S, et al. Stress, burnout and coping among emergency physicians at a major hospital in Kingston, Jamaica. West Indian Med J 2014;63:262–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Jalili M, Sadeghipour Roodsari G, Bassir Nia A. Burnout and associated factors among Iranian emergency medicine practitioners. Iran J Public Health 2013;42:1034–42. [PMC free article] [PubMed] [Google Scholar]
- [23].Julia-Sanchis R, Richart-Martinez M, Garcia-Aracil N, et al. Measuring the levels of burnout syndrome and empathy of Spanish emergency medical service professionals. Australas Emerg Care 2019;22:193–9. [DOI] [PubMed] [Google Scholar]
- [24].Kimo Takayesu J, Ramoska EA, Clark TR, et al. Factors associated with burnout during emergency medicine residency. Acad Emerg Med 2014;21:1031–5. [DOI] [PubMed] [Google Scholar]
- [25].Lloyd S, Streiner D, Shannon S. Burnout, depression, life and job satisfaction among Canadian emergency physicians. J Emerg Med 1994;12:559–65. [DOI] [PubMed] [Google Scholar]
- [26].Lu DW, Dresden S, McCloskey C, et al. Impact of burnout on self-reported patient care among emergency physicians. West J Emerg Med 2015;16:996–1001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Moukarzel A, Michelet P, Durand AC, et al. Burnout syndrome among emergency department staff: prevalence and associated factors. Biomed Res Int 2019;4:1–0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Rajan S, Engelbrecht A. A cross-sectional survey of burnout amongst doctors in a cohort of public sector emergency centres in Gauteng, South Africa. Afr J Emerg Med 2018;8:95–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Schooley B, Hikmet N, Tarcan M, et al. Comparing burnout across emergency physicians, nurses, technicians, and health information technicians working for the same organization. Medicine 2016;95:e2856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Soltanifar A, Pishbin E, Mashhadi NATTARAN, et al. Burnout among female emergency medicine physicians: a nationwide study. Emerg Med Australas 2018;30:517–22. [DOI] [PubMed] [Google Scholar]
- [31].Maslach C, Leiter MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry 2016;15:103–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Schaufeli WB, Bakker AB, Hoogduin K, et al. On the clinical validity of the Maslach burnout inventory and the burnout measure. Psychol Health 2001;16:565–82. [DOI] [PubMed] [Google Scholar]
- [33].Ziad K, Laurent B, Marianne H, et al. Burnout in French physicians: a systematic review and meta-analysis. J Affect Disord 2019;246:132–47. [DOI] [PubMed] [Google Scholar]
- [34].Yates M, Samuel V. Burnout in oncologists and associated factors: a systematic literature review and meta-analysis. Eur J Cancer Care 2019;28:e13094. [DOI] [PubMed] [Google Scholar]
- [35].Gomez-Urquiza JL, De la Fuente-Solana EI, Albendin-Garcia L, et al. Prevalence of burnout syndrome in emergency nurses: a meta-analysis. Crit Care Nurse 2017;37:e1–9. [DOI] [PubMed] [Google Scholar]