
Figure 7. Proarrhythmic effects of post-operative inflammation in patients with pre-existing substrates.
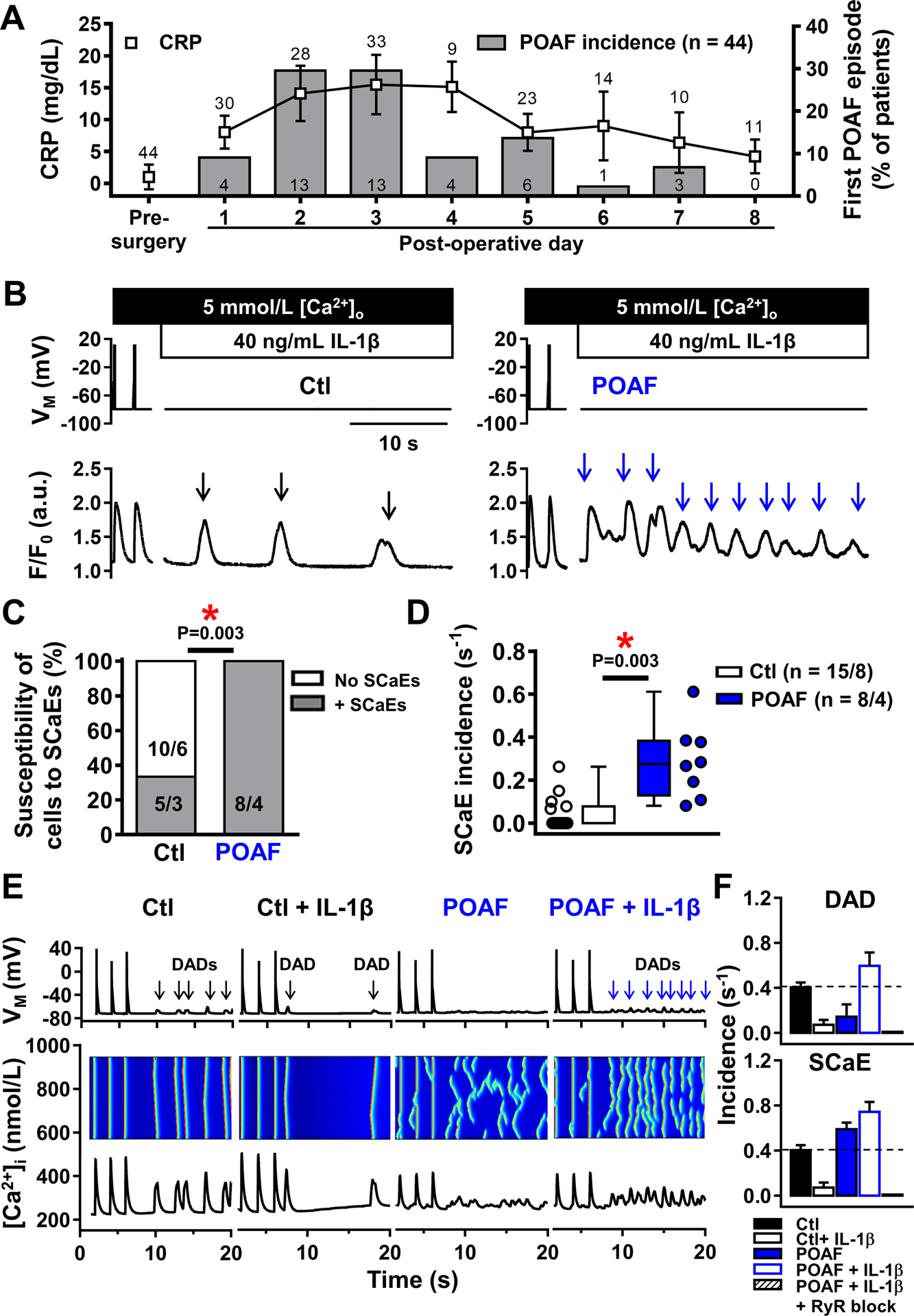
A, Coincidence of post-operative C-reactive-protein (CRP) increases (symbols) and POAF development (bars) in 44 patients with regular ECG- and CRP-measurements, showing peak incidence of POAF on days with highest CRP-levels (post-operative days 2–3). Numbers above symbols indicate number of available CRP-measurements; numbers in bars indicate absolute number of patients with a first POAF episode on a given post-operative day. B, Depolarization-induced Ca2+-transients and proarrhythmic spontaneous sarcoplasmic-reticulum Ca2+-release events (SCaEs; indicated by arrows) in a Ctl (left) and POAF (right) cardiomyocyte acutely exposed to 40-ng/mL IL-1β to mimic post-operative inflammation. C,D, Susceptibility of individual cardiomyocytes to (C) and incidence of (D) SCaEs in Ctl and POAF. One Ctl patient had one cardiomyocyte with SCaEs and one without and is therefore listed twice in panel C. E, Simulated action potentials, longitudinal line-scans and whole-cell CaTs (top-to-bottom) at 0.5-Hz and follow-up showing SCaEs and corresponding delayed afterdepolarizations (DADs) in Ctl, Ctl+IL-1β, POAF, and POAF+IL-1β models. The novel POAF human atrial cardiomyocyte model was developed by implementing the experimentally observed increases in RyR2 open-probability and SERCA function (Online Table VI). F, Quantification of SCaE (top) and DAD (bottom) incidence in 6 replications of the Ctl, Ctl+IL-1β, POAF, POAF+IL-1β and POAF+IL-1β+RyR2 block models with stochastic RyR2 gating. N-numbers indicate numbers of patients (A) or cardiomyocytes/patients (C,D). *P<0.05 vs. Ctl based on Fisher’s exact test (C) or multilevel models with log-transformed data (D).