
Figure.
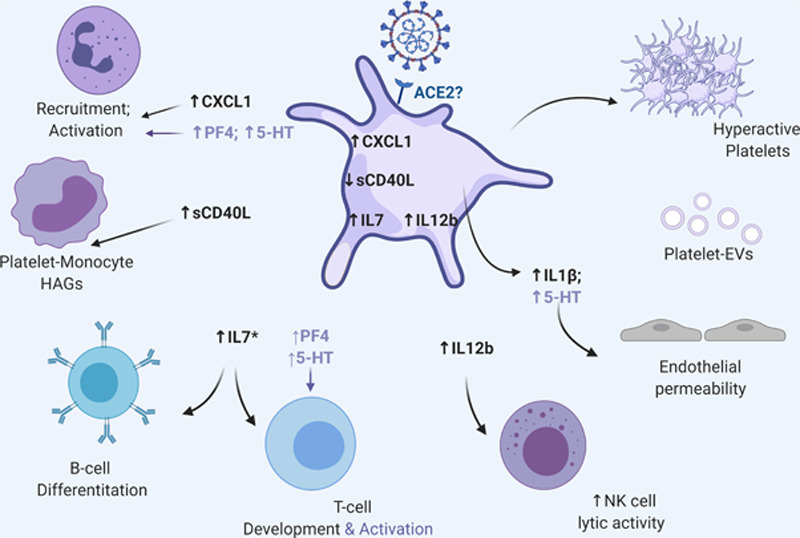
Coronavirus disease 2019 (COVID-19), platelets, and immunity. Severe acute respiratory syndrome coronavirus 2 RNA can be found in human platelets. COVID-19 changes platelet inflammatory cytokine profile important for interaction and immune cell activation. In most cases, changes in platelet cytokine level are reflected in the plasma by an undefined mechanism, and plasma levels of platelet-derived PS (phosphatidylserine)-extracellular vesicles (EVs) are also increased. Platelets from COVID-19 patients also exhibit increased baseline activation potential suggesting that they can be hyperactivated with disease severity. Hyperactivation is further reflected in the increased levels of platelet-specific granule proteins such as PF4 (platelet factor 4) and serotonin (5-HT [5-hydroxytryptamine]). PF4 and serotonin can further recruit and activate immune cells. Additionally, serotonin can increase platelet aggregation particularly in the presence of ADP, which is highly elevated during infection due to inflammasome activation and consequent cell death. Of note, in addition to the platelet-virus interactions, other signals coming from the damaged, infected, and ischemic endothelium (not depicted in this figure) can further contribute to the increased prothrombotic pathology that underlines COVID-19. This figure was generated using BioRender. ACE2 indicates angiotensin-converting enzyme 2; IL, interleukin; and sCD40L, soluble CD40 ligand.