

Abstract
Objective:
The aim is to verify the effectiveness of the pelvic floor muscle training (PFMT) program in pregnant women, by analyzing the amount of urine leakage.
Design:
Experimental study.
Location:
Care units in the Vila Real district, Portugal.
Participants:
Forty-three pregnant women divided into an experimental group (EG) (n = 22) and a control group (CG) (n = 21).
Interventions:
Both groups were evaluated in a predelivery stage (initial) and 6 months after delivery (final). The EG was given a PFMT exercise protocol with a duration of 6 weeks, applicable in classes and at home, another PFMT protocol for 9 weeks.
Main measurements:
The strength of the pelvic floor muscle was measured by the Oxford Grading Scale and the amount of urine was assessed with a Pad test. Quality of life was measured by the King's Health Questionnaire and self-efficacy by the Broome Pelvic Muscle Self-Efficacy Scale.
Results:
The loss of urine, significantly reduced from 0.86 ± 0.83 to 0.50 ± 0.67 in the EG (P = .021), whereas in the CG no significant change was observed. The degree of muscle contraction increased by 4.82 ± 0.39 in EG and 3.95 ± 0.67 in CG. The quality of life observed significant improvements in both groups (P < .05). As for self-efficacy, for the EG it improved significantly – initial (P = .001), final (P = .031), and for the CG the values remained the same.
Conclusions:
This PFMT protocol reduced urinary incontinence in pregnant women. The program allowed significant improvement in the quantity of urinary leakage and an increase in the strength of the pelvic floor muscle.
Keywords: exercise, pelvic floor muscle training, physiotherapy, pregnancy
Introduction
The International Continence Society has defined urinary incontinence (UI) as the complaint of any involuntary loss of urine1 and stress urinary incontinence (SUI) as a complaint of involuntary loss of urine caused by effort or physical exertion or sneezing or coughing.1 It is the most common type of UI in women, affecting 37% to 42%2,3 of women, being the most common type in pregnant women.4 Another study describes how 31% of UI were documented in the third trimester, with 70% of pregnant women experiencing SUI, 21.5% with mixed types, and 3.4% experiencing urge UI.5 UI is a problem with psychological repercussions in various aspects of life,6,7 which may negatively impact quality of life (QoL).8 There are several risk factors contributing toward UI, with pregnancy being one of them. This is due to the physiological and anatomical changes which occur during pregnancy.5 For the pelvic floor muscle (PFM), delivery is probably the most stressful period in a woman's lifetime3; therefore, they are at the greatest risk for stretch-related injuries.
The mechanism of UI during pregnancy is unclear, as no change is observed in the anatomy of the bladder wall or the urethra and their position within the pelvic cavity. Changes do occur in the connective tissue during pregnancy with an 8- to 10-fold increase in the collagenous fibers. The effect of hormones, especially relaxin, combined with structural changes in the pelvic support function and pressure of the pregnant uterus may contribute toward incontinence during pregnancy.5 The conservative management is the first-line treatment because of its effectiveness and lack of adverse effects.9 Several studies have concluded that pelvic floor muscle training (PFMT) is an effective therapy for SUI.10–13 PFMT can modify muscle morphology by increasing the sectional area. It also alters the neuromuscular function by increasing the ability to recruit additional motor units, as well as the frequency of arousal. In addition, it improves muscle tone and the viscoelastic properties of the connective tissue. PFMT is a progressive training program involving specificity, intensity, rest time, frequency, volume, and duration.14
The aim of this study was to verify the effectiveness of the PFMT program in pregnant women by analyzing the amount of urine leakage and observing whether incontinence symptoms improved.
Materials and methods
The study is experimental in nature, with the initial sample consisting of 43 pregnant women attending 2 community care units (CCU) in the Vila Real district, Portugal (CCU Mateus and CCU Vila Real 1) (Fig. 1). The final sample included 43 pregnant women with symptoms of SUI (but not in all pregnant women), randomly divided in 2 groups: an experimental group (EG) and a control group (CG), with 22 and 21 pregnant women, respectively (Fig. 1).
Figure 1.
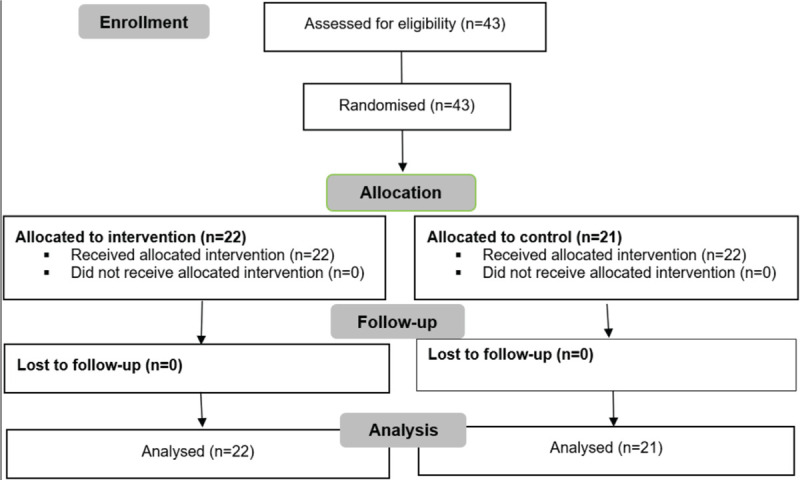
Flow diagram.
A lottery design was used for randomization of the sample, that is, 2-folded pieces of paper were placed in a common box, so that one was assigned the number 1 (CG) and the remaining was marked as number 2 (EG). It was previously agreed that the first paper that came out of the box would correspond to CCU Mateus and what remained in the box would be CCU Vila Real 1. Thus, the first draw was number 2 (EG), without knowledge of the meaning of this number, which ensured the blindness of the participants. The inclusion criteria were pregnant women, the first or second child, 28 weeks of gestation, aged 18 to 45 years. The exclusion criteria included a diagnosis of UI (urge UI and mixed UI), SUI triggered by factors external to the lower urinary tract (cognitive deficits and neurological pathologies) and pelvic organ prolapse.
Ethical approval was obtained from the North Regional Health Administration and the National Data Protection Committee. Written consent was obtained from each participant. The study was reported according to CONSORT guidelines.15
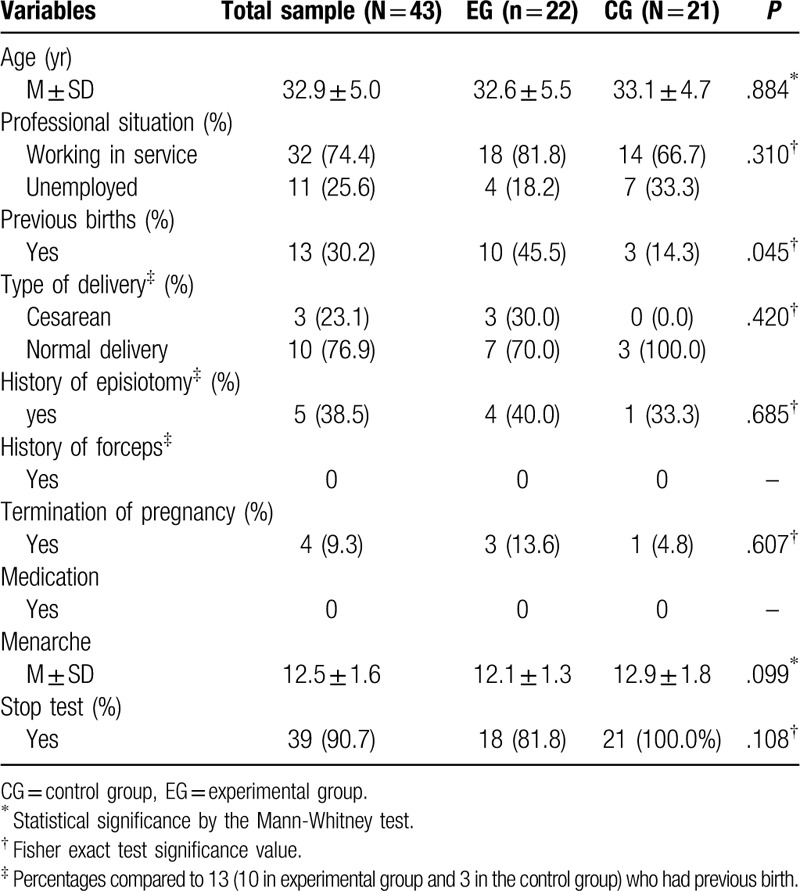
The participants’ characteristics were assessed at baseline. Demographic and clinical characteristics of the sample were collected using a questionnaire, which included age, professional situation, previous births, type of delivery, history of episiotomy, history of forceps, termination of pregnancy, medication, menarche, and stop test (Table 1).
Table 1.
Demographic and clinical characteristics of the sample (n = 43)
Intervention
All participants started their childbirth preparation classes at 28 weeks of gestation, and both groups attended the classes regularly, having their respective topics addressed by their family nurse. The only exception was that only the EG performed the PFMT protocol both at the end of class, supervised by a physiotherapist, and at home, unsupervised. All pregnant women received training with explanations regarding the general concepts of the PFM. In both groups, the primary outcomes (PFM assessment), were explained in detail, whereas the secondary outcomes (assessment of urogynecological symptoms and PFMT programs), were only explained to the EG.
Primary outcomes
Pelvic floor muscle assessment
A PFM contractility evaluation was performed by the physiotherapist at baseline and 6 months postpartum. First, a digital palpation was conducted, where the index and middle fingers were introduced 2 to 3 cm into the vaginal introitus. After a maximum contraction of the muscles, against the fingers, the muscle contractility was graded according to the Oxford Grading Scale (using the 5 point, 0 – no contraction, 5 – strong).16–18 This scale was applied by the same researcher, provide intraobserver reliability.
A Pad test (modified 20 minutes) was performed in the initial and final evaluations quantifying urine loss. It is not invasive and provides an easy, inexpensive, and objective assessment of urine loss.19
Secondary outcomes
Assessment of urogynecological symptoms
Patients of both groups completed 2 assessment questionnaires, in the initial and final phases. The Broome Pelvic Muscle Exercise Self-efficacy Scale was developed and validated by Broome20 and it was later validated for the Portuguese population by Branquinho et al. It allows for analyzing the perception of the individual of the (self) efficacy of PFM contractions.21 It is a self-administered instrument, composed of 23 items divided into 2 parts. In part A (items 1–14), participants indicate the level of confidence they feel when performing that activity without loss of urine. In part B (items 1–9), participants indicate the level of confidence they feel when performing that activity in terms of urine loss prevention.21 The scores of part A, part B, and the total scale are obtained by averaging the items involved, ranging from 0 to 100. Higher values of the scores correspond to high levels of confidence.21
The King's Health Questionnaire (KHQ) was originally developed by Kelleher et al22 and designed to assess the impact of UI on the QoL of women, also evaluating urinary symptoms and subjective measures of severity. It was recently validated for the Portuguese population having obtained a good reliability.7 It demonstrated appropriate psychometric proprieties and validity. The KHQ is composed of 21 items analyzing 3 domains and it evaluates the agreement of the subjects on a 4- and 5-option Likert scale: personal limitations and daily life, emotions, and social relations and urinary symptoms. The KHQ scored from a minimum of 0 (best QoL) to a maximum of 100 (worst QoL), scored by every domain and by their global score. Scores of an independent subscale (Symptom Severity Scale) were calculated in the same way.7
Pelvic floor muscle training programs
Exercise protocol for pelvic floor muscle in preparation classes for childbirth
This PFM protocol8,23 was applied in preparatory delivery classes, for 6 weeks (2 times/wk), consisting of 2 phases, 6 exercises each: Phase I, known as awareness/stabilization, with a duration of 3 weeks, aimed to acquire awareness and perception of the PFM, its location and ability to contract them properly, as well as create a postural and respiratory dynamics. At this stage, the progression of the exercises/positions occurred in relation to increased gravity, that is, the exercises began in the lying position and gradually evolved into a standing position; the contraction time equals the relaxation time (a 10-second interval between efforts; 10 times). The gradual progression and repetition of the contraction/relaxation movements allowed the pregnant participants to become more aware and learn to better control the action requested for each stage. Phase II, known as strength training, with a duration of 3 weeks, aimed to promote strengthening by progressively increasing muscle strength, recruiting more motor units and hypertrophy of PFM. At this stage, the contraction is greater than the relaxation time, progressively increasing the level of difficulty over time (3 exercises with 6 seconds of contraction and 3 of rest; 1 exercise with 5 seconds of contraction and 2 seconds of rest and 2 exercises with 10 seconds of contraction and 2 seconds of rest, respectively; 5 times).
Exercise protocol for pelvic floor muscle, at home
This protocol carried out at home,24 with a duration of 9 weeks, consists of 3 distinct phases, each phase lasting 3 weeks. Phase I – mixed phase, in the first and second weeks the pregnant woman must perform 10 rapid contractions (1 second) and 10 sustained contractions (5 seconds), both 3 times/day (10 seconds of relaxation); in the third week, it changes to 2 × 10 rapid contractions (1 second) and 10 sustained contractions (6 seconds), both 3 times/day (10 seconds of relaxation). Phase II –active phase, in the first and second weeks the pregnant woman must perform 2 × 10 rapid contractions (1 second) and 2 × 10 sustained contractions (7 seconds), both 3 times/day (7 seconds of relaxation); in the third week, 2 × 10 rapid contractions (1 second) and 2 × 10 sustained contractions (8 seconds), both 3 times/day (8 seconds of relaxation). Phase III – resisted phase, in the first week the pregnant woman must perform, 2 × 10 rapid contractions (2 seconds) and 3 × 10 sustained contractions (9 seconds), both 3 times/day (5 seconds of relaxation); in the second week, 2 × 10 rapid contractions (2 seconds) and 3 × 10 sustained contractions (10 seconds), both 3 times/day (5 seconds of relaxation); in the third week, 2 × 10 rapid contractions (2 seconds) and 3 × 10 sustained contractions (12 seconds), both 3 times/day (5 seconds of relaxation). Each participant will have to record their adherence to the proposed home exercise protocol on a daily basis.
Data analysis
Data were analyzed using SPSS v22.0. The variables studied were characterized by mean and standard deviation, the normal distribution of the data was tested with the Shapiro-Wilk test. This test checks the null hypothesis of a variable, following a normal distribution, and is suitable for small samples. The test results led to the conclusion that most of the variables do not have a distribution close to normal, which is a necessary condition for using parametric tests, particularly in a small sample, as is the case of this study. For the study comparing the EG and CG regarding the characteristics of participants (qualitative variables) the Fisher exact test was used. The Mann-Whitney test was used to study the significance of the difference of ages between the EG and CG. The Wilcoxon test for paired samples was used to study the significance of the differences between the initial and final phases in the EG and CG, which was done separately. The correlation between continuous variables was studied with the use of Spearman correlation coefficient.
Results
The study was carried out with 43 healthy pregnant women, aged 21 to 44 years (Fig. 1). The participants were screened and allocated to the EG (n = 22) or CG (n = 21). The participants had a mean age of 32.9 ± 5.0 years. No significant differences between the 2 groups were found in terms of baseline characteristics (P = .884) (Table 1). The participants completed the intervention and final assessments and then were included in the analysis. At the end of 9 weeks, each participant returned the protocol of adherence to the recommended exercises to be performed at home. There was 100% compliance, with no reported dropouts.
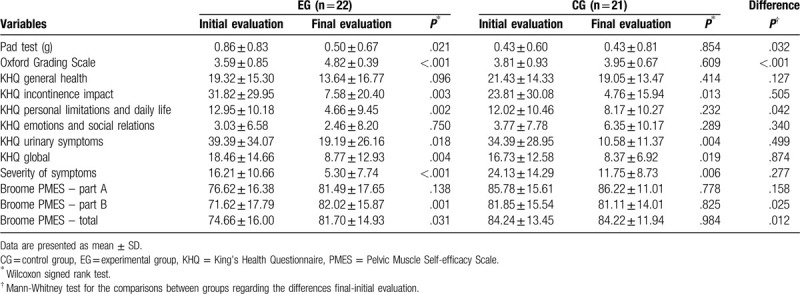
The correlation between the Pad test and the Oxford Grading Scale is not significant, both at the initial and final stages. All KHQ domains, including the KHQ global score, correlated negatively with the Oxford Scale (Table 2). The loss of urine quantified by the Pad test significantly reduced from 0.86 ± 0.83 at the initial stage to 0.50 ± 0.67 at the final stage in the EG (P = .021) but remained stable in the CG (P = .854). There were significant differences between the groups concerning the variation initial-final Pad test (P = .032) (Table 3). Therefore, there were improvements within the EG though there were no significant differences between the CG and EG. The degree of muscle contraction, measured by the Oxford scale, increased significantly in the EG (P < .001) from 3.59 ± 0.85 to 4.82 ± 0.39 and did not change significantly in the CG (P = .609) – the comparison of the differences initial-final between groups was significant (P < .001) (Table 3). The perception of general health (KHQ – general health) did not suffer any statistically significant changes between the initial and final stages in the EG (P = .096) or in the CG (P = .414). The impact of incontinence (KHQ – impact incontinence) dropped significantly from the initial to the final stage, both in the EG (P = .003) and in the CG (P = .013). For the KHQ dimensions in KHQ – personal limitations and daily life there was a significant improvement in the QoL in the EG (P = .002), but not in the CG (P = .232), with significant differences between groups regarding the variation initial-final (P = .042); in KHQ – emotions and social relations there were no significant changes either in the EG (P = .750) or in the CG (P = .289); in KHQ – urinary symptoms in size the total KHQ and severity of symptoms observed significant improvements in both groups (P < .05) (Table 3). As for the scale of Broome, in part A there were no significant changes either in the EG (P = .138) or in the CG (P = .778). In part B and the Broome-Total scale, the women in the EG improved significantly (P = .001 and P = .031, respectively), whereas in the CG there was no significant change (P > .05) – the variation initial-final differed significantly between groups in both scales (P = .025 and P = .012, respectively) (Table 3).
Table 2.
Correlational analysis between age, pad test, Oxford Grading Scale and pad test, Oxford Grading Scale, King's Health Questionnaire, and Broome Pelvic Muscle Self-efficacy Scale
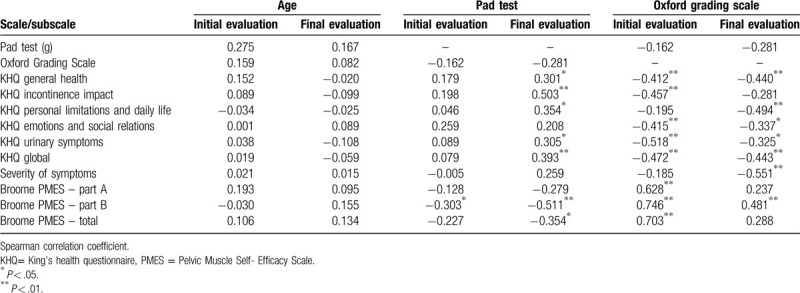
Table 3.
Comparison between initial evaluation and final evaluation in the experimental group and in the control group
Discussion
This study demonstrated that a 6-week training protocol using progressive PFMT, in combination with a 9-week home program, resulted in significant improvements in pregnant women in the EG.
UI has been considered as an injury caused by pregnancy and delivery. Several authors have studied the prevalence of UI in pregnant women and the values are identical in all studies, approximately 40%.1,2,4,25 SUI was the most common type of UI during pregnancy, with 41.7% of nulliparous women, 38% of primipara women and 20.3% of multipara women experiencing UI.25 The prevalence of SUI increased from 7% at 3 months postpartum to 30 and 42% at 5 and 12 years postpartum, respectively.26 PFMT is recommended by the International Continence Society as a means of preventing and treating pelvic floor dysfunctions,27 for being minimally invasive and without complications. PFMT is the most commonly recommended conservative therapy for pregnant women with SUI.4 The most important prognostic factor for PFMT efficacy is the adherence to the training protocol,8,28 so the EG have better results than the CG. The strength of this study includes the high adherence and implementation of an exercise program. Continue PFMT during pregnancy prevents UI during pregnancy and after delivery. PFM strength improved significantly after intensive PFMT,29 indicating that this physical condition can be improved with the practice of physical exercise. Guidelines on physical activity or exercise and pregnancy encourage pregnant women to continue or adopt an active lifestyle during and after pregnancy.30,31
The participants of the EG adhered to the program, completing it at a satisfactory level. This indicates that strength training of the PFM has to be continue to be effective, in agreement with the results of studies on women with SUI.32–34 Soave et al35 concluded in its review that the PFMT program following general strength-training principles can be recommended both during pregnancy and in the postnatal period. PFMT, combined with the physiotherapist's intervention, is increasingly becoming the first line of treatment for SUI. Physiotherapists, who use guidelines like PFMT, need to understand the nature of the SUI, the available scientific evidence, the influence of prognostic factors, and the principles of behavioral therapy. Therefore, physiotherapists may contribute to movement behavior modification and to changes in cognition about incontinence.3
Our results demonstrated that loss of urine (quantified by Pad test) significantly reduced in the EG (P = .021) and remained stable in the CG (P = .854). There were significant differences between the groups. This prevention and treatment (PFMT) was effective in reducing urine. Tosun et al36 obtained similar results in his study, the urine reduction in the PFMT group (n = 65) went from 3.1 to 0.2, after 12 weeks. The Pad test has some limitations but it is an easy, inexpensive, and objective assessment of urine loss.19 This study suggests that PFMT can reduce the incidence of SUI at gestational stages of 35 weeks and at 6 weeks and 6 months postpartum by significantly increasing PFM strength, compared with women who did not perform PFMT.4
In addition to having had consequences on the decrease of UI, this training protocol also shows an increase in the muscle strength of PFM. The degree of muscle contraction (measured by the Oxford Grading Scale) increased significantly in the EG (P < .001), from 3.59 ± 0.85 to 4.82 ± 0.39 and did not change significantly in the CG (P = .609). The comparison of the differences initial-final between groups was significant. The results for muscle strength assessed by the Oxford Grading Scale for Da Roza et al16 converge with those obtained in this study (the Oxford Scale is a reliable method to assess the PFM contraction capacity). Again, it highlights the importance of PFMT,37,38 rated grade A, with no reported side effects39 and an improvement of symptoms.38 Several studies have evaluated the muscle strength of the perineum after PFMT protocol and all had great effects in terms of increasing the strength of the PFM, either through Oxford Grading Scale or perineometry.36,40,41
The incontinence impact of the KHQ dropped significantly from the initial to final stages, both in the EG and in the CG. For the domains, KHQ (Personal limitations and daily life) there was a significant improvement in the QoL in the EG but not in the CG, with significant differences between groups regarding the variation initial-final; for KHQ (Urinary symptoms) in size, the total KHQ and severity of symptoms, significant improvements were observed in both groups (P < .05). This result shows an improvement in the UI, which improves QoL.8,14,42 Arguably, there is little value in an intervention that increases the strength of PFM if it does not also increase QoL.43,44 Other studies, which used KHQ, associated with a PFMT protocol, also demonstrated that there was an improvement in urinary symptoms and, in turn, an improvement in QoL.45,46
In the Broome Pelvic Muscle Exercise Self-efficacy Scale of PFM, there were no significant changes in part A between the EG (P = .138) and the CG (P = .778). In part B and in the total scale, the EG improved significantly (P = .001 and P = .031, respectively), whereas in the CG there was no significant change (P > .05). It was found once again that the protocol applied for 6 weeks with supervision of a physiotherapist, plus the home exercise protocol for 9 weeks, has important effects on increasing muscle strength of the PFM. Increasing PFMT increases the muscle strength.17,47 These results are similar to those of Sousa et al48 who demonstrated that self-efficacy in contracting PFM showed that the PFMT has been effective, increasing levels of self-efficacy in contraction of PFM.
The results of this research are similar to those of Dumoulin et al45 that concluded in its review that the PFMT is better than no treatment, placebo, or inactive control treatments for women with SUI. We can be confident that PFMT can cure or improve symptoms and may reduce the number of leakage episodes in women with SUI. Sousa et al48 also had findings that corroborate the results of this study. The PFMT protocol seems to be effective in UI treatment in young nulliparous athletes demonstrated a significant improvement in Pad-test, Self-efficacy of Broom, Oxford grading scale, and perineometry values, after 8 weeks protocol.
Limitations of the design
Some limitations of this study should be considered. The sample was small, the pregnant women lacked knowledge concerning SUI, not all participants were nulliparous, several participants were pregnant with their second child, and not all participants have SUI. The muscle strength of the PFM should be measured using a manometer, because it is a more reliable, accurate, and effective method. An evaluation at the end of the PFMT application was important and not just 6 months postpartum, but unfortunately it was not possible to perform it. The exercise protocol to be developed at home should also be supervised by a physiotherapist or another method should be added that proves adherence to the protocol.
This study leads to the conclusion that the PFM training program in this sample could be an effective mechanism for the prevention and reduction of urine leakage in pregnant women. The PFM training program allowed for a significant improvement of clinical symptoms in the amount of urine leakage and increased PFM strength.
Acknowledgments
None.
Author contributions
TFP: Project development, data collection, data analysis, manuscript writing; PMP: Project development, data analysis; RC: Project development, manuscript editing; RV: Project development, data collection, data analysis, manuscript editing
Conflict of interest
The authors declare no conflicts of interest.
References
- [1].Haylen BT, De Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J. 2010;21:5–26. doi:10.1007/s00192-009-0976-9. [DOI] [PubMed] [Google Scholar]
- [2].Beksac AT, Aydin E, Orhan C, et al. Gestational urinary incontinence in nulliparous pregnancy – a pilot study. J Clin Diagn Res. 2017;11:QC01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Bernards AT, Berghmans BC, Slieker-Ten Hove MC, Staal JB, De Bie RA, Hendriks EJ. Dutch guidelines for physiotherapy in patients with stress urinary incontinence: an update. Int Urogynecol J. 2014;25:171–179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Sangsawang B, Sangsawang N. Stress urinary incontinence in pregnant women: a review of prevalence, pathophysiology, and treatment. Int Urogynecol J. 2013;24:901–912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Karim R, Begum S, Ayub S, et al. Incontinence of urine in pregnant women. J Postgrad Med Institute. 2019;33:146–149. [Google Scholar]
- [6].Gil KM, Somerville AM, Cichowski S, Savitski JL. Distress and quality of life characteristics associated with seeking surgical treatment for stress urinary incontinence. Health Qual Life outcomes. 2009;7:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Viana R, Viana S, Neto F, Mascarenhas T. Adaptation and validation of the King's Health Questionnaire in Portuguese women with urinary incontinence. Int Urogynecol J. 2015;26:1027–1033. [DOI] [PubMed] [Google Scholar]
- [8].Da Roza T, De Araujo MP, Viana R, et al. Pelvic floor muscle training to improve urinary incontinence in young, nulliparous sport students: a pilot study. Int Urogynecol J. 2012;23:1069–1073. [DOI] [PubMed] [Google Scholar]
- [9].Pelaez M, Gonzalez-Cerron S, Montejo R, Barakat R. Pelvic floor muscle training included in a pregnancy exercise program is effective in primary prevention of urinary incontinence: a randomized controlled trial. Neurourol Urodyn. 2014;33:67–71. [DOI] [PubMed] [Google Scholar]
- [10].Borin LC, Nunes FR, De Oliveira Guirro EC. Assessment of pelvic floor muscle pressure in female athletes. PMR. 2013;5:189–193. [DOI] [PubMed] [Google Scholar]
- [11].Ferreira S, Ferreira M, Carvalhais A, Santos PC, Rocha P, Brochado G. Reeducation of pelvic floor muscles in volleyball athletes. Rev Assoc Med Bras. 2014;60:428–433. [Google Scholar]
- [12].Rivalta M, Sighinolfi MC, Micali S, De Stefani S, Torcasio F, Bianchi G. Urinary incontinence and sport: first and preliminary experience with a combined pelvic floor rehabilitation program in three female athletes. Health Care Women Int. 2010;31:435–443. [DOI] [PubMed] [Google Scholar]
- [13].Talasz H, Kalchschmid E, Kofler M, Lechleitner M. Effects of multidimensional pelvic floor muscle training in healthy young women. Arch Gynecol Obstet. 2012;285:709–715. [DOI] [PubMed] [Google Scholar]
- [14].B⊘ K. Urinary incontinence, pelvic floor dysfunction, exercise and sport. Sports Med. 2004;34:451–464. [DOI] [PubMed] [Google Scholar]
- [15].Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMC Med. 2010;8:18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Da Roza T, Mascarenhas T, Araujo M, Trindade V, Jorge RN. Oxford Grading Scale vs manometer for assessment of pelvic floor strength in nulliparous sports students. Physiotherapy. 2013;99:207–211. [DOI] [PubMed] [Google Scholar]
- [17].Frawley HC, Galea MP, Phillips BA, Sherburn M, B⊘ K. Reliability of pelvic floor muscle strength assessment using different test positions and tools. Neurourol Urodyn. 2006;25:236–242. [DOI] [PubMed] [Google Scholar]
- [18].Peschers U, Gingelmaier A, Jundt K, Leib B, Dimpfl T. Evaluation of pelvic floor muscle strength using four different techniques. Int Urogynecol J. 2001;12:27–30. [DOI] [PubMed] [Google Scholar]
- [19].Ferreira CHJ, B⊘ K. The Pad Test for urinary incontinence in women. J Physiother. 2015;61:98. [DOI] [PubMed] [Google Scholar]
- [20].Broome BA. Development and testing of a scale to measure self-efficacy for pelvic muscle exercises in women with urinary incontinence. Urol Nurs. 1999;19:258–268. [PubMed] [Google Scholar]
- [21].Branquinho N, Marques A, Robalo L. Contributo para a adaptação e validação do instrumento de medida “escala de auto-eficácia de Broome para exercícios da musculatura do pavimento pélvico”. EssFisiOnline. 2007;3:3–13. [Google Scholar]
- [22].Kelleher C, Cardozo L, Khullar V, Salvatore S. A new questionnaire to assess the quality of life of urinary incontinent women. Br J Obstet Gynaecol. 1997;104:1374–1379. [DOI] [PubMed] [Google Scholar]
- [23].Viana S, Viana R, Da Roza T, et al. Protocolo de exercicios dos músculos do pavimento pélvico em mulheres atletas com incontinência urinária, com aplicação de modelos biomecânicos. VIII Congresso Nacional da Associação Portuguesa de Neuro-Urologia e Uro-Ginecologia, Disfunções Miccionais, Lisboa; 2013. [Google Scholar]
- [24].Chiarapa T, Cacho D, Alves A. Physiotherapeutic treatment. Female urinary incontinence: physiotherapy and multidisciplinary assistance. 2007;Livraria Médica Paulista Editora, São Paulo: 148–153. [Google Scholar]
- [25].Dinç A. Prevalence of urinary incontinence during pregnancy and associated risk factors. Low Urin Tract Symptoms. 2018;10:303–307. [DOI] [PubMed] [Google Scholar]
- [26].Viktrup L, Rortveit G, Lose G. Risk of stress urinary incontinence twelve years after the first pregnancy and delivery. Obstet Gynecol. 2006;108:248–254. [DOI] [PubMed] [Google Scholar]
- [27].Abrams P, Andersson K, Birder L, et al. Fourth International Consultation on Incontinence Recommendations of the International Scientific Committee: evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol Urodyn. 2010;29:213–240. [DOI] [PubMed] [Google Scholar]
- [28].Chiarelli P, Murphy B, Cockburn J. Women's knowledge, practises, and intentions regarding correct pelvic floor exercises. Neurourol Urodyn. 2003;22:246–249. [DOI] [PubMed] [Google Scholar]
- [29].M⊘rkved S, B⊘ K, Schei B, Salvesen KA. Pelvic floor muscle training during pregnancy to prevent urinary incontinence: a single-blind randomized controlled trial. Obstet Gynecol. 2003;101:313–319. [DOI] [PubMed] [Google Scholar]
- [30].B⊘ K, Artal R, Barakat R, et al. Exercise and pregnancy in recreational and elite athletes: 2016 evidence summary from the IOC expert group meeting, Lausanne. Part 1—exercise in women planning pregnancy and those who are pregnant. Br J Sports Med. 2016;50:571–589. [DOI] [PubMed] [Google Scholar]
- [31].B⊘ K, Hilde G, Tennfjord MK, Sperstad JB, Engh ME. Pelvic floor muscle function, pelvic floor dysfunction and diastasis recti abdominis: Prospective cohort study. Neurourol Urodyn. 2017;36:716–721. [DOI] [PubMed] [Google Scholar]
- [32].B⊘ K, Talseth T, Holme I. Single blind, randomised controlled trial of pelvic floor exercises, electrical stimulation, vaginal cones, and no treatment in management of genuine stress incontinence in women. BMJ. 1999;318:487–493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Krhut J, Zachoval R, Smith PP, et al. Pad weight testing in the evaluation of urinary incontinence. Neurourol Urodyn. 2014;33:507–510. [DOI] [PubMed] [Google Scholar]
- [34].M⊘rkved S, B⊘ K. Effect of postpartum pelvic floor muscle training in prevention and treatment of urinary incontinence: a one-year follow up. BJOG. 2000;107:1022–1028. [DOI] [PubMed] [Google Scholar]
- [35].Soave I, Scarani S, Mallozzi M, Nobili F, Marci R, Caserta D. Pelvic floor muscle training for prevention and treatment of urinary incontinence during pregnancy and after childbirth and its effect on urinary system and supportive structures assessed by objective measurement techniques. Arch Gynecol Obstet. 2019;299:609–623. [DOI] [PubMed] [Google Scholar]
- [36].Tosun OC, Solmaz U, Ekin A, et al. Assessment of the effect of pelvic floor exercises on pelvic floor muscle strength using ultrasonography in patients with urinary incontinence: a prospective randomized controlled trial. J Phys Ther Sci. 2016;28:360–365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Dumoulin C, Hay-Smith J. Pelvic floor muscle training versus no treatment for urinary incontinence in women. A Cochrane systematic review. Eur J Phys Rehabil Med. 2008;44:47–63. [PubMed] [Google Scholar]
- [38].Price N, Dawood R, Jackson SR. Pelvic floor exercise for urinary incontinence: a systematic literature review. Maturitas. 2010;67:309–315. [DOI] [PubMed] [Google Scholar]
- [39].Morkved S. Pelvic floor muscle training during pregnancy and after delivery. Curr Women's Health Rev. 2007;3:55–62. [Google Scholar]
- [40].Pires TF, Pires PM, Moreira MH, et al. Pelvic floor muscle training in female athletes: a randomized controlled pilot study. Int J Sports Med. 2020;41:264–270. [DOI] [PubMed] [Google Scholar]
- [41].Pourkhiz Z, Mohammad-Alizadeh-Charandabi S, Mirghafourvand M, et al. Effect of Pelvic Floor Muscle Training on Female Sexual Function During Pregnancy and Postpartum: A Randomized Controlled Trial. Iran Red Crescent Med J. 2017;19:e63218.doi: 10.5812/ircmj.63218. [Google Scholar]
- [42].Fozzatti C, Riccetto C, Herrmann V, et al. Prevalence study of stress urinary incontinence in women who perform high-impact exercises. Int Urogynecol J. 2012;23:1687–1691. [DOI] [PubMed] [Google Scholar]
- [43].Dolan LM, Walsh D, Hamilton S, Marshall K, Thompson K, Ashe RG. A study of quality of life in primigravidae with urinary incontinence. Int Urogynecol J. 2004;15:160–164. [DOI] [PubMed] [Google Scholar]
- [44].Liang C-C, Wu M-P, Lin S-J, et al. Clinical impact of and contributing factors to urinary incontinence in women 5 years after first delivery. Int Urogynecol J. 2013;24:99–104. [DOI] [PubMed] [Google Scholar]
- [45].Dumoulin C, Cacciari LP, Hay-Smith EJC. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst Rev. 2018;10:CD005654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Pires T, Pires P, Moreira H, Gabriel R, Viana S, Viana R. Assessment of pelvic floor muscle in sportswomen: quality of life and related factors. Phys Ther Sport. 2020;43:151–156. [DOI] [PubMed] [Google Scholar]
- [47].B⊘ K. Pelvic floor muscle strength and response to pelvic floor muscle training for stress urinary incontinence. Neurourol Urodyn. 2003;22:654–658. [DOI] [PubMed] [Google Scholar]
- [48].Sousa M, Viana R, Viana S, et al. Effects of a pelvic floor muscle training in nulliparous athletes with urinary incontinence: biomechanical models protocol. In: Tavares J., Natal Jorge R. (eds) Computational and Experimental Biomedical Sciences: Methods and Applications. Springer, Cham, Switzerland: Lecture Notes in Computational Vision and Biomechanics. vol 21; 2015;83–90. [Google Scholar]