
Fig. 1.
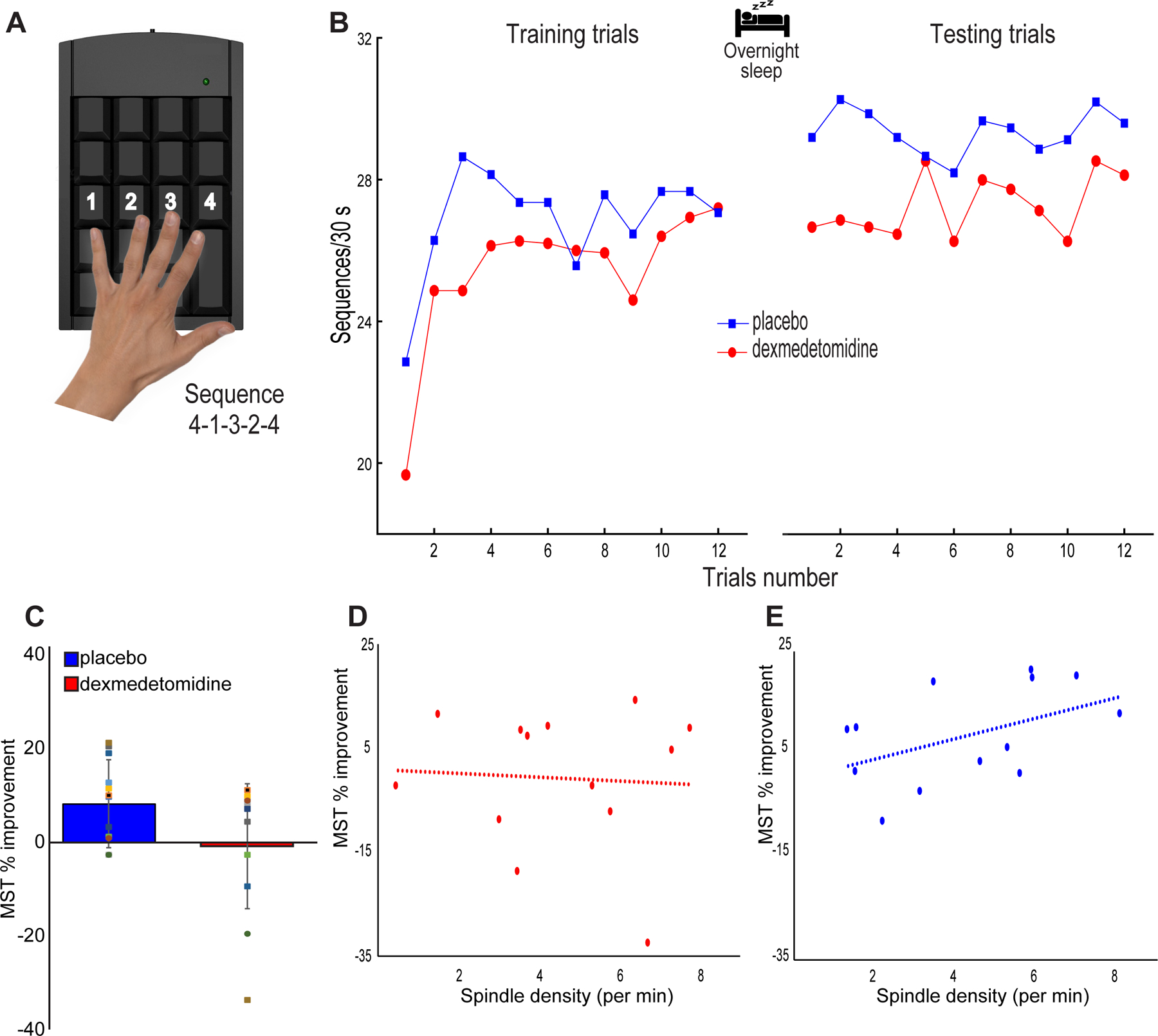
MST performance. (A) The Motor Sequence Task (MST) involves typing a 5-digit sequence (4–1–3–2–4) as quickly and correctly as possible for 12 rounds of 30 second intervals. (B) MST performance during both the placebo and dexmedetomidine study visits. Placebo visits showed visibly improved overnight performance (average of first three testing sequences - average of last three training sequences), whereas oral dexmedetomidine immediate performance appeared similar between training and testing sessions. (C) Improvement in MST performance (%) met our threshold for statistical significance for the placebo (p=0.003) but not for the dexmedetomidine (p=0.900) study visits. There were no statistically significant differences in immediate (p = 0.078) performance between groups. (D) Spindle density during non-REM stage 2 sleep and overnight MST improvement after oral dexmedetomidine were not correlated (Spearman’s Rho= 0.1, p = 0.748, n = 13; Spearman’s Rho= 0.1, p = 0.820, n = 15 after data imputation). (E) We confirmed the previously described24,26 positive correlation between spindle density during non-REM stage 2 sleep and overnight MST improvement post placebo (Spearman’s Rho= 0.54, p = 0.058, n = 13; Spearman’s Rho= 0.57, p = 0.028, n = 15 after data imputation).