
Figure 4.
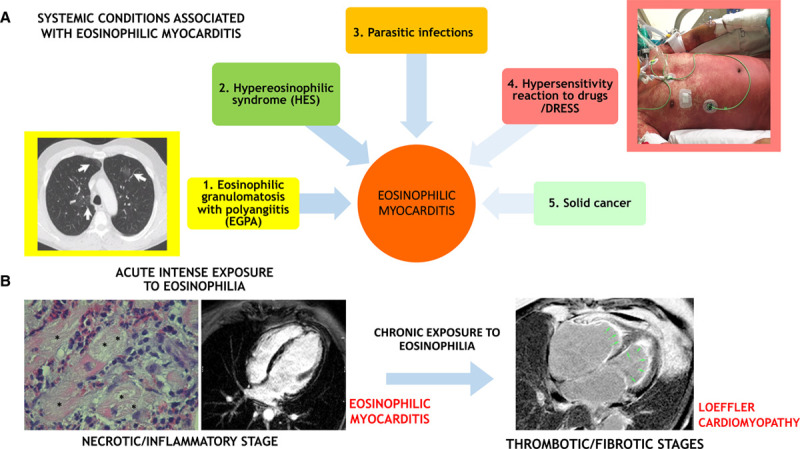
Eosinophilic myocardial injury: associated conditions and transition from acute myocarditis to inflammatory cardiomyopathy. A, Eosinophilic myocarditis can be idiopathic or associated with a systemic disorder. The associated conditions can be (1) eosinophilic granulomatosis with polyangiitis (EGPA), which is often associated with asthma, pulmonary nonfixed infiltrates (arrows on a chest computed tomographic scan image in the yellow inset), and paranasal sinus abnormalities; (2) hypereosinophilic syndromes (HES) characterized by persistent peripheral eosinophilia (≥1.5×109/L for over 6 mo), which can be a complex idiopathic form or a myeloproliferative variant like the clonal form associated with FIP1L1/PDGFRA fusion gene; (3) parasitic infections; (4) hypersensitivity reactions to drugs and drug reaction with eosinophilia and systemic symptoms (DRESS) that are generally characterized by fever and diffuse skin rush (like in the patient with DRESS showed in the rose inlet), with frequent delay onset after drug initiation (up to 2–6 wk); and rarely, (5) solid tumors. While in the acute phase, the eosinophilic myocarditis is the main determinant of prognosis, the associated conditions can be the major determinants of prognosis in the mid and long term. B, An acute intense exposure to eosinophilia can cause an acute eosinophilic myocarditis (left), which in some case can be described as necrotizing due to extensive areas of the cardiomyocyte necrosis (*) caused by diffuse eosinophilic infiltrates on endomyocardial biopsy histology. The acute inflammatory phase can cause subendocardial and transmural injuries, identified by late gadolinium enhancement on cardiac magnetic resonance imaging (CMRI). If the eosinophilic exposure persists, eosinophilic injury evolves to a thrombotic and fibrotic stage, with diffuse subendocardial fibrosis with apical thrombi (green arrows), as identified by CMRI; the latter are characteristic features of Loeffler cardiomyopathy (right).