
Figure 1.
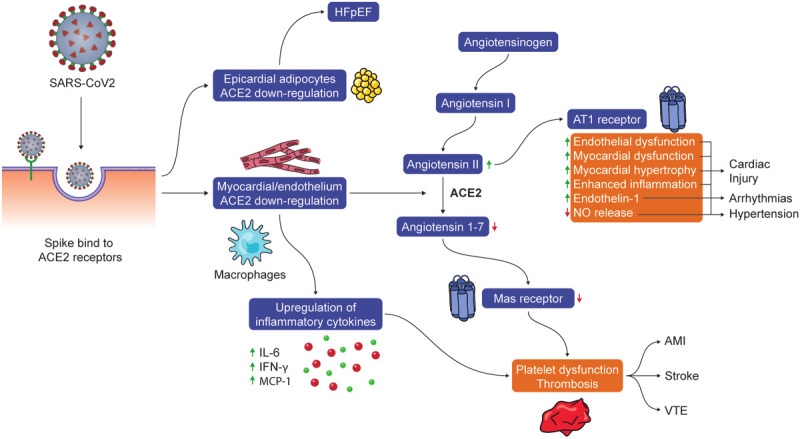
The potential pathogenesis of SARS-CoV-2 infection-related cardiovascular diseases. A spike protein of SARS-CoV-2 has high susceptibility in individuals who have increased ACE2 gene expression (e.g., pre-existing CVD), leading a downregulation of ACE2. ACE2 downregulation could result in the upregulation of inflammatory cytokines (e.g., IL-6), a reduction in the degradation of angiotensin II, and decreased angiotensin 1-7. Decreased angiotensin 1-7 could lead to subsequent decreased activation of Mas receptors on platelets which in combination of inflammatory cytokine upregulation (e.g. IL-6, IFN-, MCP-1) may result in acquired platelet dysfunction and intravascular thrombosis. Additionally, increased angiotensin II mediated AT1 receptor activation may have multiple physiologic effects including myocardial hypertrophy and dysfunction, interstitial fibrosis, endothelial dysfunction, enhanced inflammation, increased endothelin-1 expression and decreased NO release which can manifest as cardiac injury, arrhythmias and hypertension.