

Abstract
A growing body of studies has demonstrated that acute transcranial magnetic stimulation (TMS) therapy for treatment-resistant major depressive disorder (MDD) has achieved significant antidepressant effects and can alleviate other related symptoms. However, MDD has a high relapse rate, and patients with depressive symptoms can relapse weeks or months after acute TMS treatment. The lack of necessary TMS maintenance protocols after completing acute TMS treatment with full remission might be one of the reasons for the high relapse rates in MDD patients. Thus, investigating post-TMS treatment maintenance guidelines is important for decreasing relapse in treatment-resistant depression patients who had initially responded to acute TMS therapy. Therefore, we recommend a scientific approach to decrease relapse in treatment-resistant depression patients who had initially responded to acute TMS treatment.
Keywords: Transcranial magnetic stimulation, major depressive disorder, depression, acute, maintenance, treatment-resistant, therapy
Introduction
Major depressive disorder (MDD) is a chronic or recurrent psychiatric disorder that is associated with high morbidity, and presents as a big financial burden [1]. Accumulating evidence has suggested that 48% of patients suffering from depression have had suicidal thoughts, and 24% of those have attempted suicide. Furthermore, many patients report not receiving or even recognizing the need for treatment [2]. In addition, research has shown that the incidence of suicide is highest during MDD episodes [2].
An early report on the relapse of MDD shows a high relapse rate after 12 weeks, with the majority of patients relapsing after four weeks [3]. Increasing evidence supports the notion that for many people suffering from depression, relapse after initial recovery is almost a habitual pattern [4]. The likelihood of future depressive episodes can be as high as 30%, and this rate can increase with each subsequent episode [2].
Acute TMS therapy for patients with depression
A growing body of studies has demonstrated that acute transcranial magnetic stimulation (TMS) therapy for treatment-resistant MDD has achieved significant antidepressant effects and can help alleviate other related symptoms [5-7]. Currently, a large amount of evidence supports the conclusion that high frequency TMS of the left dorsolateral prefrontal cortex (DLPFC) and low frequency TMS of the right DLPFC exert antidepressant effects on MDD, especially in the acute phase of monophasic depressive episodes [8-10]. In conventional clinical practice, TMS was shown to be effective for the acute treatment of MDD, and the statistical and clinical significance of the improvement was manifested in the MDD patients reported quality of life and functional status [6]. After acute TMS therapy for six weeks without adjustment for depression severity, the predictive rate of suicidal ideation was significantly reduced in adolescents who had treatment-resistant depression (TRD) [5]. Another study on TRD found that repetitive TMS (rTMS) provided significant benefits in short-term treatment for patients with TRD [10].
However, MDD has a high relapse rate, and patients with depressive symptoms can relapse weeks or months after acute TMS treatment. Depressed patients (n=204) treated with rTMS were enrolled into the follow-up study of Cohen et al [11]. According to their findings, 80% of the patients relapsed after successful rTMS treatment [11]. In addition, some studies have found that after acute TMS therapy for MDD, the antidepressant effects gradually decreased, followed by a tendency of relapse [12]. Therefore, it is important to investigate different post-TMS maintenance guidelines for MDD patients who had initially responded to an acute phase of rTMS treatment to try and decrease relapse.
Maintenance TMS therapy for patients with depression
Several studies have investigated the use of certain maintenance rTMS to decrease relapse of TRD after acute treatment with rTMS. A study on MDD discovered that almost 30% of patients had decreased symptoms after acute and daily TMS for 3 weeks [13]. Moreover, acute deep TMS (dTMS) for four weeks induced a 6.39 point improvement in the Hamilton Depression Rating Scale (HDRS-21) scores. The antidepressant effects also remained stable over three months of dTMS maintenance treatment in MDD outpatients who had either failed one to four antidepressant trials or had not tolerated at least two antidepressant treatments during a current episode [14]. In addition, HDRS-6 scores showed significant reductions during 21 weeks of maintenance TMS therapy in treatment-resistant MDD patients who had responded to at least two courses of acute TMS treatment over four weeks and had experienced relapse within three months following the second to last successful acute treatment course [15] (See Table 1 for details).
Table 1.
Summary of studies on the effects of maintenance TMS in depression patients responding to acute TMS treatment
| Subjects | Types of depression | Antidepressant-free during TMS Treatment | The course of depression | Duration of TMS Treatment (weeks) | TMS treatment effects | References | ||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| Acute phase | Maintenance phase | Acute phase | Maintenance phase | |||||
| Adults (n=43) | BD I/II | N | an acute depressive episode | 4 | 4 | HDRS-17 scores ↓ | HDRS-17 scores ⇡ | [2] |
| Patients (n=16) | Unipolar, treatment-resistant MDD | Y | single or recurrent type | 6 | 44 | HDRS-17 scores | HDRS-17 scores ⇣ | [20] |
| Outpatients (n=120) | Unipolar nonpsychotic MDD | Y | single or recurrent type | 3 | 3 | HAMD scores ↓ | Almost 30% of patients remitted | [24] |
| Outpatients (n=71) | MDD | Y | the current episode | 4 | 12 | HDRS-21 scores ↓ | Improvement in HDRS-21 scores is stable | [6] |
| Patients (n=39) | MDD | N | Remission/Partial | 4 | 21 | HAMD6 scores ↓ | After TMS series, 79% patients were in remission | [13] |
| Remission/Relapse | ||||||||
| Patients (n=17) | Unipolar/bipolar TRD | N | Partial Remission/Relapse | 4 | 44 | HDRS-17 scores ↓ | HDRS-17 scores (only in the fourth month) ↓ | [19] |
BD, bipolar depression; MDD, major depressive disorder; ↓, it represents a significant decrease in certain symptoms; ⇡, it represents a nonsignificant increase in certain scores; ⇣, it represents a nonsignificant decrease in certain scores; HDRS-17/21, 17/21-item Hamilton Depression Rating Scale; HAMD, Hamilton Scale for Depression; TRD, treatment-resistant depression; Y, yes; N, no.
In a study on the maintenance of TMS treatment for a relatively long time (53 weeks), after antidepressant-free patients with unipolar, non-psychotic, treatment-resistant MDD underwent six weeks of acute TMS, these patients were randomized to receive either a scheduled, single TMS session delivered monthly (SCH) or placed in observation-only regimens (OBS). Patients given SCH therapy revealed a longer time to relapse compared to the patients in OBS, but there was no statistical significance as compared to the control group (OBS) [16]. Tavares et al reported that active dTMS was superior to placebo surgery, but it was not effective in the maintenance phase (week eight) after four weeks of acute dTMS treatment for resistant bipolar depression patients [12] (See Table 1 for details). Thus, it can be seen that TMS maintenance therapy is not always able to prevent relapse in treatment-resistant MDD. Whether maintenance TMS therapy can prevent relapse of MDD may be related to the frequency and duration of its use and the attenuation cycle of TM antidepressant effects. Benadhira et al reported that of the 58 TRD patients who received rTMS for one month in an open-label study (phase I), 35 of the patients responded to the acute rTMS therapy. Afterwards, 17 patients were randomized to receive maintenance sessions (phase II) for the subsequent eleven months, characterized by gradually reducing the regularity of the rTMS sessions [17] (See Figure 1 for details). The delta HDRS scores demonstrated a significant improvement between the first month and the fourth month for the active group compared to the placebo group (phase II) [17]. This TMS frequency of gradually reducing the regularity of rTMS sessions may be a step toward a scientific approach to decreasing or preventing relapse in TRD patients who had initially responded to acute TMS treatment. In addition, the implementation of maintenance TMS therapy can be affected by many other factors, such as medical reimbursement. One study comparing electroconvulsive therapy (ECT) to TMS found that due to ECT having more side effects, TRD patients may prefer TMS treatment if TMS is included in the service list of the health maintenance organization [18].
Figure 1.
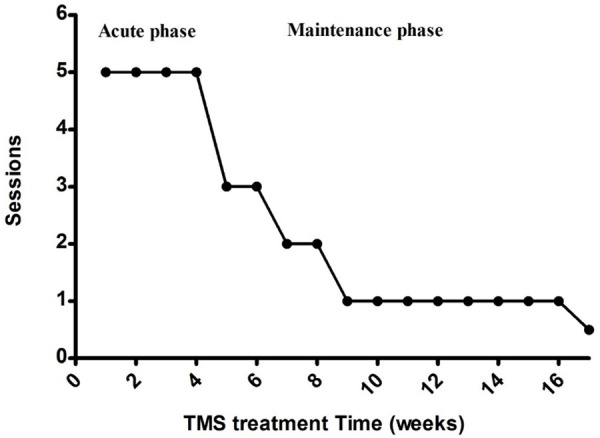
A scientific regimen of maintenance TMS treatment for treatment-resistant MDD patients who had initially responded to acute TMS treatment. In the first month of phase 1 (acute phase), all participants were treated with TMS. During maintenance rTMS treatment (maintenance phase), the regularity of rTMS sessions was gradually reduced as follows: three sessions per week for two weeks, followed by two sessions per week for the next two weeks, followed by one session per week for two months, followed by one session every two weeks for eight months. Data in the figure was collected from the reference [17].
Possible mechanisms of TMS on MDD
The antidepressant mechanisms of TMS are highly relevant to the monoamine neurotransmitter systems, the amino acid transmitter systems, and the cortical circuits with abnormal baseline functional connectivity in depression [19]. For example, TMS treatment elevated prefrontal cortex γ-aminobutyric acid in MDD patients [20]. In addition, Iwabuchi et al demonstrated that the therapeutic effects of rTMS may be modulated by the right anterior insula through using targeted intermittent theta-burst stimulation [21]. Similarly, acute rTMS of the left DLPFC in healthy volunteers modulated aspects of tryptophan/serotonin metabolism in the limbic areas, including the left para-hippocampal gyrus, the right insula, the right cingulate gyrus, and the cuneus [22]. There is evidence that rTMS has the potential to alleviate symptoms that may be related to functional abnormalities in the frontocingulate circuit in some patients with MDD [23]. Future studies are warranted to explore the cellular and molecular mechanisms of TMS on MDD.
Conclusion
The research on acute TMS treatment for treatment-resistant MDD has influenced the development of maintenance TMS treatment guidelines for depression, especially to help decrease or prevent relapse in treatment-resistant MDD patients who had initially responded to acute TMS treatment. TMS, unlike many therapies in medicine, does not suffer from an efficacy/effectiveness gap between clinical trials and clinical treatments. The lack of necessary TMS maintenance protocols after completing acute TMS treatment with full remission may be one of the reasons for the high relapse rates in MDD patients [24]. Therefore, maintenance TMS therapy in line with scheduled TMS frequency attenuation may effectively reduce or prevent the relapse of MDD in treatment-resistant MDD patients who had initially responded to acute TMS treatment.
Acknowledgements
This work was partly supported by grants from Qiqihar Medical University (QY2016-ZD1), Heilongjiang Province, China, the University of Missouri Research Board, Missouri, USA and American Heart Association (19AIREA34470007) to XPC.
Disclosure of conflict of interest
None.
References
- 1.McMahon EM, Buszewicz M, Griffin M, Beecham J, Bonin EM, Rost F, Walters K, King M. Chronic and recurrent depression in primary care: socio-demographic features, morbidity, and costs. Int J Family Med. 2012;2012:316409. doi: 10.1155/2012/316409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Richards D. Prevalence and clinical course of depression: a review. Clin Psychol Rev. 2011;31:1117–1125. doi: 10.1016/j.cpr.2011.07.004. [DOI] [PubMed] [Google Scholar]
- 3.Keller MB, Shapiro RW, Lavori PW, Wolfe N. Relapse in major depressive disorder: analysis with the life table. Arch Gen Psychiatry. 1982;39:911–915. doi: 10.1001/archpsyc.1982.04290080031005. [DOI] [PubMed] [Google Scholar]
- 4.Mueller TI, Leon AC, Keller MB, Solomon DA, Endicott J, Coryell W, Warshaw M, Maser JD. Recurrence after recovery from major depressive disorder during 15 years of observational follow-up. Am J Psychiatry. 1999;156:1000–1006. doi: 10.1176/ajp.156.7.1000. [DOI] [PubMed] [Google Scholar]
- 5.Croarkin PE, Nakonezny PA, Deng ZD, Romanowicz M, Voort JLV, Camsari DD, Schak KM, Port JD, Lewis CP. High-frequency repetitive TMS for suicidal ideation in adolescents with depression. J Affect Disord. 2018;239:282–290. doi: 10.1016/j.jad.2018.06.048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Janicak PG, Dunner DL, Aaronson ST, Carpenter LL, Boyadjis TA, Brock DG, Cook IA, Lanocha K, Solvason HB, Bonneh-Barkay D, Demitrack MA. Transcranial magnetic stimulation (TMS) for major depression: a multisite, naturalistic, observational study of quality of life outcome measures in clinical practice. CNS Spectr. 2013;18:322–332. doi: 10.1017/S1092852913000357. [DOI] [PubMed] [Google Scholar]
- 7.Sehatzadeh S, Daskalakis ZJ, Yap B, Tu HA, Palimaka S, Bowen JM, O’Reilly DJ. Unilateral an bilateral repetitive transcranial magnetic stimulation for treatment-resistant depression: a meta-analysis of randomized controlled trials over 2 decades. J Psychiatry Neurosci. 2019;44:151–163. doi: 10.1503/jpn.180056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.George MS, Taylor JJ, Short EB. The expanding evidence base for rTMS treatment of depression. Curr Opin Psychiatry. 2013;26:13–18. doi: 10.1097/YCO.0b013e32835ab46d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lefaucheur JP, Andre-Obadia N, Antal A, Ayache SS, Baeken C, Benninger DH, Benaderette S, Camdessanché JP, Cassereau J, Convers P, d’Anglejean J, Delval A, Durand MC, Etard O, Fayet G, Fournier E, Franques J, Gavaret M, Guehl D, Guerit JM, Krim E, Kubis N, Lacour A, Lozeron P, Mauguière F, Merle PE, Mesrati F, Mutschler V, Nicolas G, Nordine T, Pautot V, Péréon Y, Petiot P, Pouget J, Praline J, Salhi H, Trébuchon A, Tyvaert L, Vial C, Zola JM, Zyss J, Lefaucheur JP. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS) Clin Neurophysiol. 2014;125:2150–2206. doi: 10.1016/j.clinph.2014.05.021. [DOI] [PubMed] [Google Scholar]
- 10.Lam RW, Chan P, Wilkins-Ho M, Yatham LN. Repetitive transcranial magnetic stimulation for treatment-resistant depression: a systematic review and metaanalysis. Can J Psychiatry. 2008;53:621–631. doi: 10.1177/070674370805300909. [DOI] [PubMed] [Google Scholar]
- 11.Cohen RB, Boggio PS, Fregni F. Risk factors for relapse after remission with repetitive transcranial magnetic stimulation for the treatment of depression. Depress Anxiety. 2009;26:682–688. doi: 10.1002/da.20486. [DOI] [PubMed] [Google Scholar]
- 12.Tavares DF, Myczkowski ML, Alberto RL, Valiengo L, Rios RM, Gordon P, de Sampaio-Junior B, Klein I, Mansur CG, Marcolin MA, Lafer B, Moreno RA, Gattaz W, Daskalakis ZJ, Brunoni AR. Treatment of bipolar depression with deep TMS: results from a double-blind, randomized, parallel group, sham-controlled clinical trial. Neuropsychopharmacology. 2017;42:2593–2601. doi: 10.1038/npp.2017.26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.George MS, Lisanby SH, Avery D, McDonald WM, Durkalski V, Pavlicova M, Anderson B, Nahas Z, Bulow P, Zarkowski P, Holtzheimer PE 3rd, Schwartz T, Sackeim HA. Daily left prefrontal transcranial magnetic stimulation therapy for major depressive disorder: a sham-controlled randomized trial. Arch Gen Psychiatry. 2010;67:507–516. doi: 10.1001/archgenpsychiatry.2010.46. [DOI] [PubMed] [Google Scholar]
- 14.Levkovitz Y, Isserles M, Padberg F, Lisanby SH, Bystritsky A, Xia G, Tendler A, Daskalakis ZJ, Winston JL, Dannon P, Hafez HM, Reti IM, Morales OG, Schlaepfer TE, Hollander E, Berman JA, Husain MM, Sofer U, Stein A, Adler S, Deutsch L, Deutsch F, Roth Y, George MS, Zangen A. Efficacy and safety of deep transcranial magnetic stimulation for major depression: a prospective multicenter randomized controlled trial. World Psychiatry. 2015;14:64–73. doi: 10.1002/wps.20199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pridmore S, Erger S, Rybak M, Kelly E, May T. Early relapse (ER) transcranial magnetic stimulation (TMS) in treatment resistant major depression. Brain Stimul. 2018;11:1098–1102. doi: 10.1016/j.brs.2018.05.013. [DOI] [PubMed] [Google Scholar]
- 16.Philip NS, Dunner DL, Dowd SM, Aaronson ST, Brock DG, Carpenter LL, Demitrack MA, Hovav S, Janicak PG, George MS. Can medication free, treatment-resistant, depressed patients who initially respond to TMS be maintained off medications? A prospective, 12-month multisite randomized pilot study. Brain Stimul. 2016;9:251–257. doi: 10.1016/j.brs.2015.11.007. [DOI] [PubMed] [Google Scholar]
- 17.Benadhira R, Thomas F, Bouaziz N, Braha S, Andrianisaina PS, Isaac C, Moulier V, Januel D. A randomized, sham-controlled study of maintenance rTMS for treatment-resistant depression (TRD) Psychiatry Res. 2017;258:226–233. doi: 10.1016/j.psychres.2017.08.029. [DOI] [PubMed] [Google Scholar]
- 18.Magnezi R, Aminov E, Shmuel D, Dreifuss M, Dannon P. Comparison between neurostimulation techniques repetitive transcranial magnetic stimulation vs electroconvulsive therapy for the treatment of resistant depression: patient preference and cost-effectiveness. Patient Prefer Adherence. 2016;10:1481–1487. doi: 10.2147/PPA.S105654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dubin M. Imaging TMS: antidepressant mechanisms and treatment optimization. Int Rev Psychiatry. 2017;29:89–97. doi: 10.1080/09540261.2017.1283297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dubin MJ, Mao X, Banerjee S, Goodman Z, Lapidus KA, Kang G, Liston C, Shungu DC. Elevated prefrontal cortex GABA in patients with major depressive disorder after TMS treatment measured with proton magnetic resonance spectroscopy. J Psychiatry Neurosci. 2016;41:E37–45. doi: 10.1503/jpn.150223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Iwabuchi SJ, Raschke F, Auer DP, Liddle PF, Lankappa ST, Palaniyappan L. Targeted transcranial theta-burst stimulation alters fronto-insular network and prefrontal GABA. Neuroimage. 2017;146:395–403. doi: 10.1016/j.neuroimage.2016.09.043. [DOI] [PubMed] [Google Scholar]
- 22.Sibon I, Strafella AP, Gravel P, Ko JH, Booij L, Soucy JP, Leyton M, Diksic M, Benkelfat C. Acute prefrontal cortex TMS in healthy volunteers: effects on brain 11C-alphaMtrp trapping. Neuroimage. 2007;34:1658–1664. doi: 10.1016/j.neuroimage.2006.08.059. [DOI] [PubMed] [Google Scholar]
- 23.Paus T, Barrett J. Transcranial magnetic stimulation (TMS) of the human frontal cortex: implications for repetitive TMS treatment of depression. J Psychiatry Neurosci. 2004;29:268–279. [PMC free article] [PubMed] [Google Scholar]
- 24.Malik S, Malik A, Mercille K. 79 failure to do maintenance therapy after completion of transcranial magnetic stimulation treatment is a cause of relapse of depression in MDD Patient. CNS Spectr. 2019;24:215. [Google Scholar]