
Fig. 1.
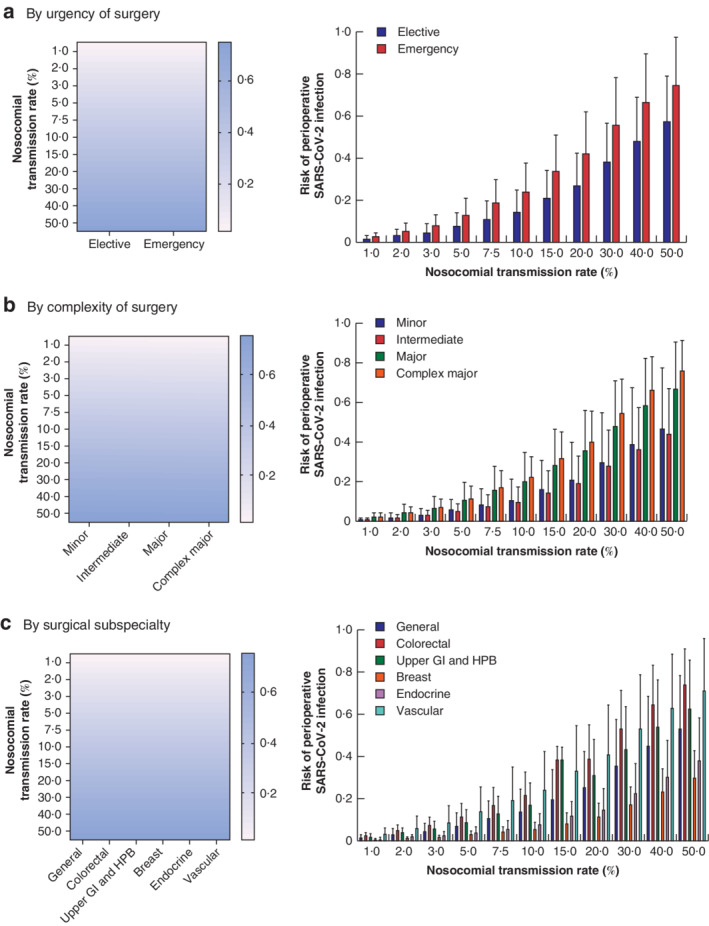
Nosocomial transmission rate and estimated postoperative SARS-CoV-2 infection risk
a By urgency of surgery, b by complexity of surgery and c by surgical subspecialty. a Emergency procedures were associated with an increased risk of nosocomial SARS-CoV-2 infection compared with elective procedures (P < 0·001), with the greatest risk at higher nosocomial transmission rates (P < 0·001 for interaction). b The risk of postoperative SARS-CoV-2 infection was significantly associated with procedural complexity, with the greatest risk following major surgery (P < 0·001 versus intermediate, P = 0·044 versus minor) and complex major surgery (P = 0·033 versus major, P < 0·001 versus intermediate, P < 0·001 versus minor). The impact of procedural complexity was greater at increased nosocomial transmission rates (P < 0·001 for interaction). c Surgical subspecialty was a significant factor in terms of risk of perioperative SARS-CoV-2 (P < 0·001). The greatest risk of SARS-CoV-2 infection was observed for general, colorectal, vascular and upper gastrointestinal (GI) and hepatobiliary (HPB) procedures. Breast and endocrine procedures were associated with a significantly reduced risk of nosocomial SARS-CoV-2 infection compared with all other subspecialties (P < 0·050) (mixed-effects analysis with post hoc Tukey multiple comparisons test).