
Fig. 2.
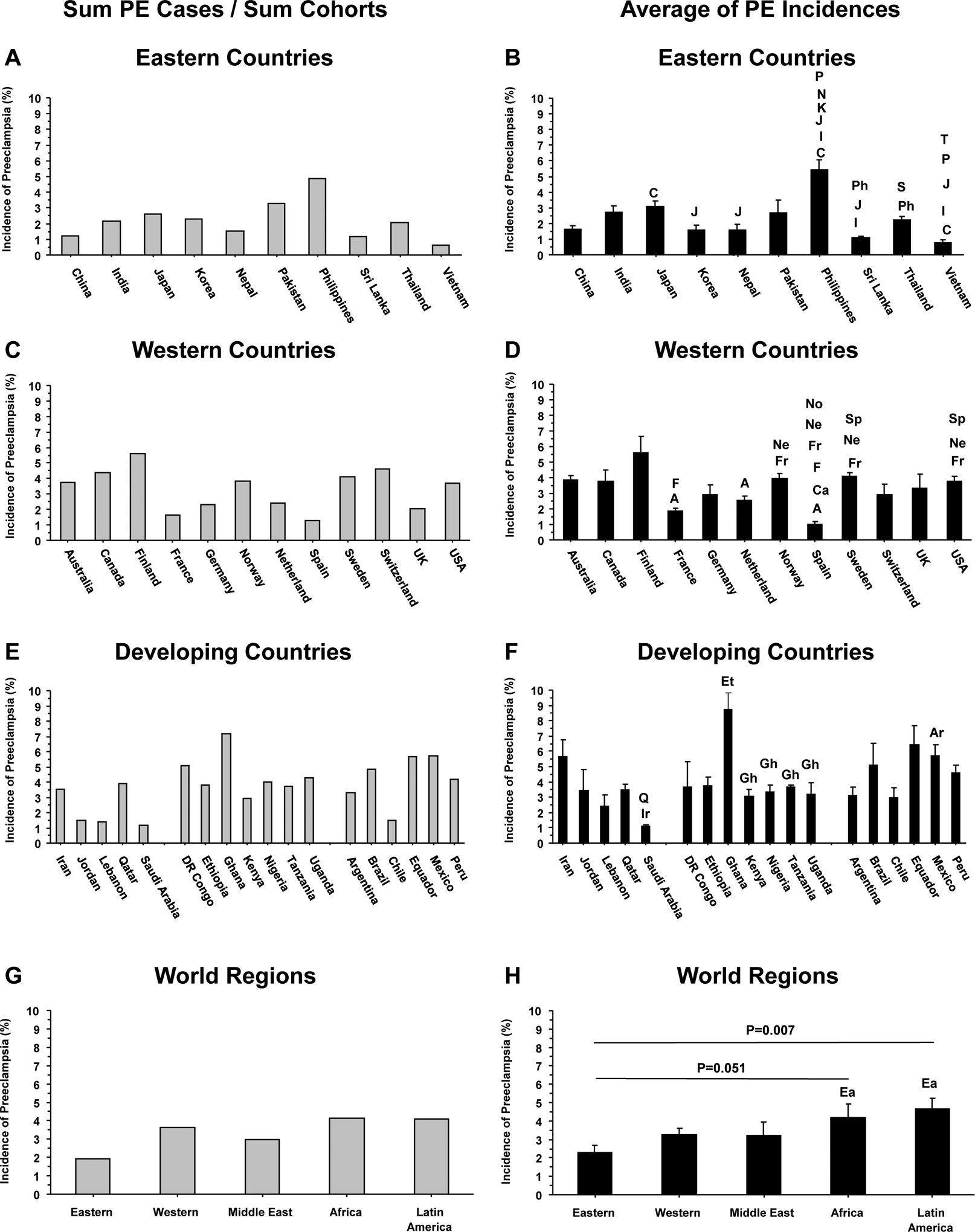
Average incidence of PE in representative countries and in the Eastern Western and Developing world. Data from the 4 studies presented in Figure 1 were used to calculate the average incidence of PE in representative countries and world regions by dividing the Sum number of PE cases by the Sum number of pregnant women in the different cohorts (A, C, E and F), or by calculating the means±SEM of the incidences of PE from the 4 different studies, which allowed statistical comparison of different countries and regions (B, D, F and H). Letters on columns indicate significantly different (p<0.05) from C (China), I (India), J (Japan), K (Korea), N (Nepal), P (Pakistan), Ph (Philippines), S (Sri Lanka), and (T) Thailand in Eastern Countries (B); significantly different (p<0.05) from A (Australia), Ca (Canada), F (Finland), Fr (France), Ne (Netherland), No (Norway), Sp (Spain) in Western Countries (D); significantly different (p<0.05) from Ir (Iran), and Q (Datar) in the Middle East, from Et (Ethiopia), and Gh (Ghana) in Africa, and from Ar (Argentina) in Latin America (F); and borderline (p=0.051) or significantly different (p=0.007) from Ea (Eastern world) in different world regions (H).