

Abstract
Introduction
Most studies investigate sexual dysfunction in drug abusers; however, there are no data available about the pattern of drug abuse in patients with lifelong premature ejaculation (PE).
Aim
To assess the pattern of drug abuse in patients with lifelong PE and to evaluate its potential effect on their hormonal profile.
Methods
A cross-sectional study included patients with lifelong PE (n = 76) with no prescribed medications for 1 month and age-matched control without PE (n = 48). Participants were evaluated by history, examination, Arabic index of PE, and hormonal profile. A urine sample was screened by dipstick kits for the following drug abuse tramadol, opiate, tetrahydrocannabinol (cannabis), amphetamine, barbiturate, cocaine, and benzodiazepines. Positive results were confirmed with a immunoassay drug analyzer.
Main outcome measures
The outcomes of this study are positive and negative drug abuse and hormonal profile changes.
Results
Control patients and patients with PE showed median (interquartile range) of age 43 (33–46.8) and 38.5 (31–45) years, respectively. Drug abuse testing results showed significantly high positive drug abuse in patients with PE, 26 of 76 (34.2%), in comparison with control, 9 of 48 (19.1%) (P = .05). The most commonly abused drug was tetrahydrocannabinol in control, 3 of 9 (33.3%), and tramadol, 12 of 26 (46.2%), in patients with PE. Control patients and patients with PE with positive drug abuse had significantly higher smoking percent (P < .0001) and higher positive drug abuse history (P < .0001). However, there was no relationship between drug abuse and PE severity, and there were no significant changes in their hormonal profile.
Conclusions
Drug abuse is high among patients with lifelong PE in Upper Egypt, with tramadol being the comment drug. Drug abuse is common among smokers. However, no hormonal disturbance could be shown in drug abuse patients. Drug abuse might be considered in the evaluation of patients with PE.
Mohammed SA, Abdelhamed A, El Sayed RM. Evaluation of Drug Abuse in Patients With Lifelong Premature Ejaculation: A Cross-Sectional Study. Sex Med 2020;8:608–614.
Key Words: Drug Abuse, Lifelong Premature Ejaculation, Tramadol Abuse, Male Hormonal Profile
Introduction
Drug abuse is defined by the harmful or hazardous use of psychoactive substances, including alcohol and illicit drugs. The repeated use of these psychoactive substances can lead to dependence syndrome, which leads to a strong desire to have the drug, inability to control its use, and continue its use despite negative consequences.1 There is a great diversity in drug abuse prevalence and attitudes among different countries due to cultural and socioeconomic factors.2 In Egypt, drug abuse is considered a serious health problem due to its spread among youths, with tramadol being the commonest drug and cigarette smoking with marijuana is the commonest practice.3
Although many patients with sexual dysfunction are often using illicit drugs as aphrodisiacs for enhancement of their sexual performance, the current data suggest the negative impact of most of these illicit drugs on sexual functions.4,5 High rates of sexual dysfunction have been reported in opioid addicts 34–85%, with erectile dysfunction (ED) and premature ejaculation (PE) are the commonest ones.6 PE prevalence is 3 times higher in opiate-dependent men than the general population. The presence of PE might be a potential risk factor for relapse of opiate abuse as many patients believed the beneficial effect of opiate on PE.7 Opioid could increase sexual dysfunction in a dose-dependent pattern.8 In addition, it seems that cannabis may impair erectile function in animal and in vitro studies.9 In a community survey evaluating the sexual dysfunction and drug abuse, painful sex and inhibited orgasm were associated with marijuana use.10
However, most studies are focusing on evaluating sexual dysfunctions in drug abusers, and no data are available about screening drug abuse in patients with sexual dysfunction especially PE. Therefore, this cross-sectional study was designed to assess the pattern of drug abuse in patients with lifelong PE; in addition, to identify the relationship between drug abuse and PE severity and to evaluate the impact of drug abuse on the hormonal profile in PE patients.
Materials and methods
Design and Setting
A cross-sectional study was conducted on male patients with PE (n = 76) seeking medical advice at the andrology outpatient clinic, Sohag University Hospital, Sohag, Egypt, in the period from January 2017 to October 2019. Age-matched controls without PE (n = 48) were investigated in the study. Healthy controls were recruited from blood transfusion donors. The study design was approved by the Ethical and Scientific Research Committee of Sohag University. Written informed consent was obtained from all participants. The study included patients with lifelong PE aged between 18 and 55 years without a history of other types of sexual dysfunction for at least 6 months. Diagnosis of lifelong PE was performed as per the International Society for Sexual Medicine criteria, which were the rapid ejaculation with self-estimated intravaginal ejaculation latency time less than 1 minute; with lack of patient control on his ejaculation; and the presence of negative psycho-social consequences.11 Patients with the following conditions were excluded: diabetes mellitus, hypertension, history of advanced kidney or liver diseases, history of chronic pain, history of endocrine disorders including hypogonadism, history of other sexual dysfunction, history of psychotropic drug use, and history of prescribed medications of PE for 1 month before the study.
I. Initial Evaluation
History taking of sexual dysfunction patients included personal history, special habits, drug treatment, and sexual history. General examination included body weight, height, and body mass index, followed by a genital examination.
II. PE Evaluation
The Arabic Index of PE (AIPE) was used to evaluate participants. It is a validated diagnostic tool for PE. The total score of responses to each of the 7 items on the AIPE can range from 1 to 35, with lower scores indicating severe PE. As per to the AIPE, PE severity was classified into 5 categories; severe (7–13), moderate (14–19), mild to moderate (20–25), mild (26–30), and no PE (31–35).12
III. Laboratory Investigations
III-A- Screening for drug abuse in urine specimen
III- A- 1. Rapid dipstick
Screening tests for drug abuse in urine samples was performed by dipstick named ABON Multi-Drug that is a 1-step screen test panel used for the qualitative detection of drugs of abuse, which includes (tramadol, opiate, tetrahydrocannabinol (THC), amphetamine, barbiturate, benzodiazepines), and the test was considered positive (when there was a colored line in the control line region [C] and a colored line in the test line region [T] for a specific drug), negative (when there was a colored line in the control line region [C] but no line in the test line region [T] for a specific drug), or invalid (when there was no line in the control line region [C]).
III- A- 2. Confirmation by the drug analyzer
Positive results were confirmed by a immunoassay drug analyzer (CDx90; Thermo Fisher Scientific Co, Supplier AMG Company). The analysis was carried out at the Clinical Toxicological Laboratory, Sohag University Hospital, Sohag, Egypt. This assay uses a specific antibody that can detect most drugs of abuse and their metabolites in urine. The assay is based on the competition of enzyme glucose-6-phosphate dehydrogenase labeled drug and the free drug in the urine sample for the fixed amount of antibody binding sites. In the absence of the free drug in the sample, the enzyme-labeled drug is bound by the specific antibody, and enzyme activity is inhibited. This phenomenon creates a relationship between drug concentration in urine and enzyme activity. The enzyme (glucose-6-phosphate dehydrogenase) activity is determined at 340 nm spectrophotometrically by its ability to convert nicotinamide adenine dinucleotide (NAD+) to its reduced form which is the NADH.
III-B- Hormonal assessment
A morning blood sample was withdrawn at (8:00–10:00 am) in plain tubes. The samples centrifuged at 3,500 rpm for 5 minutes to obtain serum for hormonal assessment including total testosterone, luteinizing hormone, and follicle-stimulating hormone. Serum samples were tested on the MINI VIDAS apparatus (bioMérieux Clinical Diagnostics) to measure the needed hormones. It is a compact automated immunoassay system based on the enzyme-linked fluorescent assay principle.
Sample Size Calculation
Sample size calculation was carried out using the following formula13: , where z is the standard normal variate at 5% type of error (P < .05), P is the expected prevalence from the literature (5–10%), and d is the absolute precision of 5%. The adequate sample size was estimated from 65 to 124. So, 124 participants were included (76 patients with PE and 48 non-PE control).
Statistical Analysis
Data were analyzed by using SPSS (Statistical Package for Social Science), version 24, software. Continuous variables were expressed as the median and interquartile range. Categorical variables were expressed as percentages. Kolmogorov-Smirnov was used for testing the normality of the variables. For continuous variables, a comparison between 2 normally distributed variables was performed with independent samples t-test, whereas the Mann-Whitney U test was used to compare between 2 not normally distributed variables. For categorical variables, the chi-square test was used. P-value ≤ .05 was considered significant.
Results
The study included 76 patients with PE and 48 healthy control with median age (interquartile range) of 38.5 (31–45) and 43 (33–46.8) years, respectively. More than half of patients with PE (51.3%) and control (54.2%) were smokers, with no history of alcohol intake. The average PE duration was 11.5 (8–18) months. Patients with a positive history of illicit drug abuse were 41.7% in control and 43.4% in patients with PE, with average drug abuse durations in control and patients with PE were 5.5 (4.5–10) and 4 (2.3–6) years, respectively. All patients had a normal genital examination. All data related to the patients’ characteristics including history, general examination, and laboratory investigations were summarized in Table 1. There was no significant difference between control and patients with PE except the AIPE that was significantly lower in patients with PE, 18 (16–23), as compared with control, 33 (31–34) (P = .003), as shown in Table 1.
Table 1.
Clinical and laboratory characteristics of control (n = 48) and patients with premature ejaculation (n = 76)
| Parameter | Control n = 48 Median (IQR) or percentage |
Premature ejaculation n = 76 Median (IQR) or percentage |
P-value |
|---|---|---|---|
| History: | |||
| Age (y) | 43(33–46.8) | 38.5(31–45) | .41 |
| Smoking (%) | 54.2% | 51.3% | .82 |
| Smoking duration (y) | 14 (12.5–25) | 15 (11–20) | .56 |
| Cigarette/day | 20 (17.5–30) | 20 (15–30) | .42 |
| Brinkman smoking index | 280 (175–540) | 300 (220–510) | .87 |
| Occupation: | .53 | ||
| Manual worker/farmer | 50% | 53.9% | |
| Employee | 29.2% | 34.2% | |
| Driver | 20.8% | 11.8% | |
| Sexual history: | |||
| Frequency of intercourse/wk | 2 (2–3) | 3 (3–3) | .37 |
| Wife age (y) | 37 (25.7–41) | 31 (27–39) | .27 |
| Drug abuse history: | |||
| Positive illicit drug abuse history | 41.7% | 43.4% | .88 |
| Drug abuse duration (y) | 5.5 (4.5–10) | 4 (2.3–6) | .37 |
| Route of drug administration: | .18 | ||
| Oral | 30% | 62.4% | |
| Inhalation | 40% | 18.6% | |
| Oral/Inhalation | 30% | 18.8% | |
| General examination: | |||
| Weight (Kg) | 75 (70–89) | 78 (72–86) | .82 |
| Height (M) | 1.6 (1.6–1.7) | 1.6 (1.6–1.7) | .75 |
| BMI (Kg/m2) | 23.4 (20.7–25.7) | 23.4 (21.8–25.7) | .81 |
| Hormonal profile: | |||
| Total testosterone (ng/mL) | 6.42 (2.9–7.8) | 6.24 (2.7–7.6) | .81 |
| LH (mIU/mL) | 3(1.9–4.8) | 3.1 (2.1–5) | .81 |
| FSH (mIU/mL) | 3.6 (1.8–5.6) | 3.5 (1.9–4.7) | .69 |
| Premature ejaculation evaluation: | |||
| AIPE | 33 (31–34) | 18 (16–23) | .003 |
Bold indicates significant P-value ≤.05.
AIPE = Arabic index of premature ejaculation; BMI = body mass index; FSH = follicle stimulating hormone; IQR = interquartile range; LH = luteinizing hormone.
After using the dipsticks for drug abuse screening in urine, 11 of 48 (22.9%) control and 28 of 76 (36.8%) patients with PE were positive for drug abuse. All positive drug abuse results were confirmed by the drug analyzer. The false positive results were observed in 2 of 48 (4.2%) control and 2 of 76 (2.6%) of patients with PE. Drug abuse testing results showed significantly high positive drug abuse in 26 of 76 patients with PE (34.2%) in comparison with 9 of 48 control patients (19.1%) (P = .05). The final result of drug abuse testing and the number of abused drugs/patients is summarized in Table 2.
Table 2.
Comparison between control (n = 48) and patients with premature ejaculation (n = 76) as per the result of drug abuse
| Parameter | Control n = 48 n (percentage) |
Premature ejaculation n = 76 n (percentage) |
P-value |
|---|---|---|---|
| Drug abuse testing result: | |||
| Positive | 9 (19.1%) | 26 (34.2%) | .05 |
| Negative | 38 (80.9%) | 50 (65.8%) | |
| Number of abused drug/patient | |||
| Single drug abuse | 6 (66.7%) | 21 (80.8%) | .38 |
| Multiple drug abuse | 3 (33.3%) | 5 (19.2%) |
Bold indicates significant P-value ≤.05.
The most commonly abused drug was THC in 3 of 9 control patients (33.3%) and tramadol in 12 of 26 patients with PE (46.2%). The percentage of different types of drug abuse in all control and patients with PE is shown in Figure 1. History of drug abuse and smoking was significantly higher in positive drug abuse vs negative drug abuse in both control and patients with PE groups (P < .0001). However, there was no significant difference between positive and negative drug abuse in both control and patients with PE groups as regards the degree of AIPE and the hormonal profile as shown in Table 3.
Figure 1.
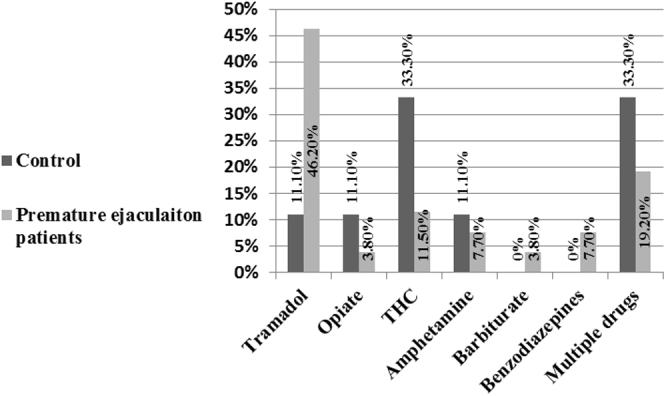
The percentage of different types of drug abuse in all control and patients with PE. PE = premature ejaculation.
Table 3.
Comparison of smoking, drug abuse history, Arabic index of premature ejaculation (AIPE), and the hormonal profile in control and patients with premature ejaculation as per the result of drug abuse testing
| Variables | Control n = 48 Median (IQR) |
Premature ejaculation n = 76 Median (IQR) |
||||
|---|---|---|---|---|---|---|
| Negative drug abuse n = 39 | Positive drug abuse n = 9 | P | Negative drug abuse n = 50 | Positive drug abuse n = 26 | P | |
| Smoking (%) | 0% (0/39) | 100% (9/9) | <.0001 | 30% (15/50) | 92.3% (24/26) | <.0001 |
| History of drug abuse (%) | 13.3% (5/39) | 88.9% (8/9) | <.0001 | 20% (10/50) | 88.5% (23/26) | <.0001 |
| AIPE | 33 (31–34) | 32.5 (31–33.5) | .51 | 18 (16–23) | 18.5 (16–22.5) | .85 |
| Total testosterone (ng/mL) | 6.6 (3.7–8.6) | 4.1 (1.9–7) | .78 | 6.2 (2.6–7.7) | 5.5 (2.6–7.5) | .45 |
| LH (mIU/mL) | 3.6 (2.4–5.1) | 2.1 (1.7–3) | .65 | 3.3 (2.4–5) | 2.7 (1.9–5) | .36 |
| FSH (mIU/mL) | 4.3 (2.2–5.6) | 2.4 (1.7–5.6) | .38 | 4.2 (2.5–5.6) | 2.7 (1.8–4) | .28 |
Bold indicates significant P-value ≤.05.
FSH = follicle stimulating hormone; IQR = interquartile range; LH = luteinizing hormone.
Discussion
Most of the current literature support that drug abuse has a negative influence on sexual functions although lack of clear underlying mechanisms.5 This negative influence could not be reversed immediately by stopping drug abuse.14 The present study tries to evaluate drug abuse among patients with lifelong PE in Upper Egypt. In the present study, drug abuse was significantly higher in 26 of 76 patients with PE (34.2%) in comparison with 9 of 48 controls (19.1%). Tramadol was the most commonly abused drug in 12 of 26 patients with PE (46.2%), whereas THC was the commonest one among 3 of 9 controls (33.3%). The high prevalence of tramadol abuse in the present study could be the demand of patients with PE to control their ejaculation as tramadol exhibit efficacy in controlling ejaculation.15 Moreover, patients who abuse drugs are more likely to suffer from PE through a higher degree of anxiety in those patients, which patients who abuse drugs to continue their abuse to control their PE.16 Patients who abuse opioid usually experience short but very intense euphoria followed by the release of tension that might delay ejaculation,17 and opioid withdrawal has been associated with PE recurrence.18 Therefore, patients who abuse drugs refuse to stop the abuse because of their feeling of the positive effects of the drug on sexual behavior. This issue should be considered in the drug abuse treatment program to enhance its success.19
In a cross-sectional study among men who will later become a drug abuser, PE prevalence was 37.5%, suggesting the potential link between PE and drug abuse.20 It must be noted that the pattern of drug abuse in patients with PE was reported in the present study, but this is a quite different from substance use disorders that require specific criteria over 12 months as per the Diagnostic and Statistical Manual of Mental Disorders-5.21
In the current study, tramadol was the commonest drug abused among patients with PE in comparison with control. Tramadol is mainly an opioid receptor agonist with some monoaminergic reuptake inhibitory activity. It is used in acute and chronic pain therapy; however, its abrupt cessation increases the incidence of withdrawal symptoms.22 In a systematic review, on-demand tramadol treatment is considered effective in improving intravaginal ejaculation latency time and satisfaction in patients with PE. It shows fair safety especially with lower doses (25–50 mg).23 Although tramadol efficacy is demonstrated in PE therapy, the tramadol dependence potential is the main concern. However, there is a lack of evidence supporting the negative impact of tramadol abuse on libido, erectile function, and testosterone level.15
It is usually assumed that there is a great difference in the prevalence and pattern of drug abuse studies owing to different study groups and different methodologies.2 Tramadol abuse was among 18 of 204 (8.8%) Egyptian school students (13–18 years of age), and a high association with smoking was found.24 This was lower than the present study result. It could seem that tramadol abuse is increased with age as our prevalence was in 26 of 76 patients with PE (34.2%) aged 38.5(31–45) years. It must be noted that large numbers of Egyptian men have misconceptions as regards the efficacy of tramadol in improving physical and sexual well-being. An Egyptian cohort study evaluated married men during tramadol dependence, and 6 months after the complete stoppage of tramadol, revealed that most of the myths of tramadol values were proved to be wrong.25 However, a large community survey in Egypt involving 44,000 subjects using a questionnaire derived from the Addiction Severity Index showed the drug abuse lifetime prevalence was 7.2–14.5%, with cannabis was the commonest drug followed by alcohol.26
For testing drug abuse, different specimens can be obtained including body fluids such as urine, blood, saliva, and sweat. Other specimens can be obtained from hair, breath, and meconium. These different specimens exhibit different detection windows for drug abuse owing to different rates and durations of excretion. Urine testing for drug abuse has a short to an intermediate window of detection (up to 30 days). However, these rapid urine tests lack specificity and should be confirmed by specific antibodies.27
In the present study, smoking was significantly higher in positive drug abuse in both patients with PE and control. This was found also among Egyptian adolescent students. The relationship between drug abuse especially tramadol and smoking are bidirectional. The smoking increases tramadol abuse and tramadol abuse increases the nicotine dependence.24,28 So, smoking could be a gateway for drug abuse.29 Based on this finding, reducing smoking could be a possible solution for controlling the drug abuse problem. However, it should be noted that the present study pointed to the significant association between smoking and drug abuse in patients with PE, but there is no proof of the causation relationship.
In the present study, there were no significant changes in the hormonal profile between positive and negative drug abuse in both patients with PE and control groups. However, another study evaluated patients who are opioid-dependent (n = 30) and found low testosterone with high prolactin and luteinizing hormone.30 This difference may be due to those patients in the present study who were not drug-dependent as in this previous study. In addition, the lower number of patients in the previous study is another limitation of its result.
In the present study, there were no significant changes in the severity of PE between positive and negative drug abuse in both patients with PE and control groups. This could be due to the small sample size. In addition, this could be due to the high level of anxiety in patients with PE, which force then to continue abuse to alleviate their anxiety regardless of the degree of PE severity.16 However, sexual dysfunction could be one of the important reasons to start drug abuse as some patients believe that drug abuse could improve their sexuality problem. Therefore, drug abuse prevalence has been increased with increased sexual dysfunction severity.31 Because of the close relationship between drug abuse and sexuality in the concept of the patients with sexual dysfunction especially PE, they usually declare their drug abuse history when discussing their sexual problems with a physician. This could explain our finding in the present study that drug abuse history shows significant changes between positive and negative drug abuse in both patients with PE and control groups.
Other reasons for drug abuse in addition to sexual improvement could include relaxation, being intoxicated, being awake at night, and enhancing a specific activity.32 Risky sexual behaviors have been reported more in men with drug abuse including anal intercourse, less condom use, and having sex with a casual partner.33 In addition, drug abuse is associated with increased HIV risk.34 However, the link between sex under the influence of drug and sexual risk behavior has not been supported in heterosexual men in another study.35
The study has several limitations. The sample size was limited. There were great difficulties in recruiting healthy control in the study. A large number of healthy controls refused to be checked for drug abuse owing to social and legal concerns. In addition, the cost of drug abuse testing was the main limiting factor. In addition, results of drug abuse testing were confirmed using the drug analyzer that is qualitative to denote the presence or absence of the drug, but no concentration for the drug was measured. Therefore, a large sample sized study with more healthy control is recommended. In addition, it will be interesting to compare patients with different drug abuse doses to evaluate the dose-dependent effects of these drugs.
Conclusions
Drug abuse is high among patients with lifelong PE in Upper Egypt, with tramadol being the common drug. Drug abuse is common among smokers. However, no hormonal disturbance could be shown in patients with drug abuse. Drug abuse might be considered in the evaluation of patients with PE.
Statement of authorship
Soheir A. Mohammed, Amr Abdelhamed, Reda M. El Sayed: Writing - Original Draft, Formal Analysis, Conceptualization, Methodology, Investigation, Resources, Writing - Review & Editing, Funding Acquisition, Project Administration.
Footnotes
Conflict of Interest: The authors report no conflicts of interest.
Funding: None.
References
- 1.Zou Z., Wang H., d'Oleire Uquillas F. Definition of substance and non-substance addiction. Adv Exp Med Biol. 2017;1010:21–41. doi: 10.1007/978-981-10-5562-1_2. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization . World Health Organization; Geneva: 2010. ATLAS on substance use: (2010): resources for the prevention and treatment of substance use disorders. [Google Scholar]
- 3.Loffredo C.A., Boulos D.N., Saleh D.A. Substance use by Egyptian youth: current patterns and potential avenues for prevention. Subst Use Misuse. 2015;50:609–618. doi: 10.3109/10826084.2014.997391. [DOI] [PubMed] [Google Scholar]
- 4.Kumsar N.A., Kumsar Ş., Dilbaz N. Sexual dysfunction in men diagnosed as substance use disorder. Andrologia. 2016;48:1229–1235. doi: 10.1111/and.12566. [DOI] [PubMed] [Google Scholar]
- 5.Zaazaa A., Bella A.J., Shamloul R. Drug addiction and sexual dysfunction. Endocrinol Metab Clin North Am. 2013;42:585–592. doi: 10.1016/j.ecl.2013.06.003. [DOI] [PubMed] [Google Scholar]
- 6.Grover S., Mattoo S.K., Pendharkar S. Sexual dysfunction in patients with alcohol and opioid dependence. Indian J Psychol Med. 2014;36:355–365. doi: 10.4103/0253-7176.140699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chekuri V., Gerber D., Brodie A. Premature ejaculation and other sexual dysfunctions in opiate dependent men receiving methadone substitution treatment. Addict Behav. 2012;37:124–126. doi: 10.1016/j.addbeh.2011.08.005. [DOI] [PubMed] [Google Scholar]
- 8.Ajo R., Segura A., Inda M.M. Opioids increase sexual dysfunction in patients with non-cancer pain. J Sex Med. 2016;13:1377–1386. doi: 10.1016/j.jsxm.2016.07.003. [DOI] [PubMed] [Google Scholar]
- 9.Shamloul R., Bella A.J. Impact of cannabis use on male sexual health. J Sex Med. 2011;8:971–975. doi: 10.1111/j.1743-6109.2010.02198.x. [DOI] [PubMed] [Google Scholar]
- 10.Johnson S.D., Phelps D.L., Cottler L.B. The association of sexual dysfunction and substance use among a community epidemiological sample. Arch Sex Behav. 2004;33:55–63. doi: 10.1023/B:ASEB.0000007462.97961.5a. [DOI] [PubMed] [Google Scholar]
- 11.Serefoglu E.C., McMahon C.G., Waldinger M.D. An evidence-based unified definition of lifelong and acquired premature ejaculation: report of the Second International Society for Sexual Medicine Ad Hoc Committee for the definition of premature ejaculation. J Sex Med. 2014;11:1423–1441. doi: 10.1111/jsm.12524. [DOI] [PubMed] [Google Scholar]
- 12.Arafa M., Shamloul R. Development and evaluation of the Arabic index of premature ejaculation (AIPE) J Sex Med. 2007;4:1750–1756. doi: 10.1111/j.1743-6109.2006.00213.x. [DOI] [PubMed] [Google Scholar]
- 13.Charan J., Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35:121–126. doi: 10.4103/0253-7176.116232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Vallejo-Medina P., Sierra J.C. Effect of drug use and influence of abstinence on sexual functioning in a Spanish male drug-dependent sample: a multisite study. J Sex Med. 2013;10:333–341. doi: 10.1111/j.1743-6109.2012.02977.x. [DOI] [PubMed] [Google Scholar]
- 15.Abdel-Hamid I.A., Andersson K.E., Waldinger M.D. Tramadol abuse and sexual function. Sex Med Rev. 2016;4:235–246. doi: 10.1016/j.sxmr.2015.10.014. [DOI] [PubMed] [Google Scholar]
- 16.Del Rio F.J., Cabello-Garcia M.A., Cabello-Santamaria F. [Effects of drug use and anxiety on premature ejaculation in a sample of Spanish drug addicts] Rev Int Androl. 2018;16:159–166. doi: 10.1016/j.androl.2017.09.004. [DOI] [PubMed] [Google Scholar]
- 17.Mirin S.M., Meyer R.E., Mendelson J.H. Opiate use and sexual function. Am J Psychiatry. 1980;137:909–915. doi: 10.1176/ajp.137.8.909. [DOI] [PubMed] [Google Scholar]
- 18.Mintz J., O'Hare K., O'Brien C.P. Sexual problems of heroin addicts. Arch Gen Psychiatry. 1974;31:700–703. doi: 10.1001/archpsyc.1974.01760170088014. [DOI] [PubMed] [Google Scholar]
- 19.Bosma-Bleeker M.H., Blaauw E. Substance use disorders and sexual behavior; the effects of alcohol and drugs on patients' sexual thoughts, feelings and behavior. Addict behaviors. 2018;87:231–237. doi: 10.1016/j.addbeh.2018.07.005. [DOI] [PubMed] [Google Scholar]
- 20.La Pera G., Franco Giannotti C., Taggi F. Prevalence of sexual disorders in those young males who later become drug abusers. J Sex Marital Ther. 2003;29:149–156. doi: 10.1080/713847172. [DOI] [PubMed] [Google Scholar]
- 21.Hasin D.S., O'Brien C.P., Auriacombe M. DSM-5 criteria for substance use disorders: recommendations and rationale. Am J Psychiatry. 2013;170:834–851. doi: 10.1176/appi.ajp.2013.12060782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Miotto K., Cho A.K., Khalil M.A. Trends in tramadol: pharmacology, metabolism, and misuse. Anesth Analg. 2017;124:44–51. doi: 10.1213/ANE.0000000000001683. [DOI] [PubMed] [Google Scholar]
- 23.Kirby E.W., Carson C.C., Coward R.M. Tramadol for the management of premature ejaculation: a timely systematic review. Int J Impot Res. 2015;27:121–127. doi: 10.1038/ijir.2015.7. [DOI] [PubMed] [Google Scholar]
- 24.Bassiony M.M., Salah El-Deen G.M., Yousef U. Adolescent tramadol use and abuse in Egypt. Am J Drug Alcohol Abuse. 2015;41:206–211. doi: 10.3109/00952990.2015.1014959. [DOI] [PubMed] [Google Scholar]
- 25.El-Hadidy M.A., El-Gilany A.-H. Physical and sexual well-being during and after tramadol dependence. Middle East Curr Psychiatry. 2014;21:148–151. [Google Scholar]
- 26.Hamdi E., Gawad T., Khoweiled A. Lifetime prevalence of alcohol and substance use in Egypt: a community survey. Subst Abus. 2013;34:97–104. doi: 10.1080/08897077.2012.677752. [DOI] [PubMed] [Google Scholar]
- 27.Hadland S.E., Levy S. Objective testing: urine and other drug tests. Child Adolesc Psychiatr Clin N Am. 2016;25:549–565. doi: 10.1016/j.chc.2016.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bassiony M.M., Abdelghani M., Salah El-Deen G.M. Opioid use disorders attributed to tramadol among Egyptian University students. J Addict Med. 2018;12:150–155. doi: 10.1097/ADM.0000000000000380. [DOI] [PubMed] [Google Scholar]
- 29.Lai S., Lai H., Page J.B. The association between cigarette smoking and drug abuse in the United States. J Addict Dis. 2000;19:11–24. doi: 10.1300/J069v19n04_02. [DOI] [PubMed] [Google Scholar]
- 30.Abdelazim S., Abolmagd S.F., Abdalla H. Sexual dysfunction and sex hormone levels in Egyptian opioid-dependent males. Am J Pharm Health Res. 2015;3:81–91. [Google Scholar]
- 31.La Pera G., Carderi A., Marianantoni Z. Sexual dysfunction prior to first drug use among former drug addicts and its possible causal meaning on drug addiction: preliminary results. J Sex Med. 2008;5:164–172. doi: 10.1111/j.1743-6109.2007.00571.x. [DOI] [PubMed] [Google Scholar]
- 32.Boys A., Marsden J., Strang J. Understanding reasons for drug use amongst young people: a functional perspective. Health Educ Res. 2001;16:457–469. doi: 10.1093/her/16.4.457. [DOI] [PubMed] [Google Scholar]
- 33.Calsyn D.A., Cousins S.J., Hatch-Maillette M.A. Sex under the influence of drugs or alcohol: common for men in substance abuse treatment and associated with high risk sexual behavior. Am J Addict. 2010;19:119–127. doi: 10.1111/j.1521-0391.2009.00022.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Meade C.S., Bevilacqua L.A., Moore E.D. Concurrent substance abuse is associated with sexual risk behavior among adults seeking treatment for prescription opioid dependence. Am J Addict. 2014;23:27–33. doi: 10.1111/j.1521-0391.2013.12057.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Calsyn D.A., Baldwin H., Niu X. Sexual risk behavior and sex under the influence: an event analysis of men in substance abuse treatment who have sex with women. Am J Addict. 2011;20:250–256. doi: 10.1111/j.1521-0391.2011.00123.x. [DOI] [PMC free article] [PubMed] [Google Scholar]