
Fig. 4.
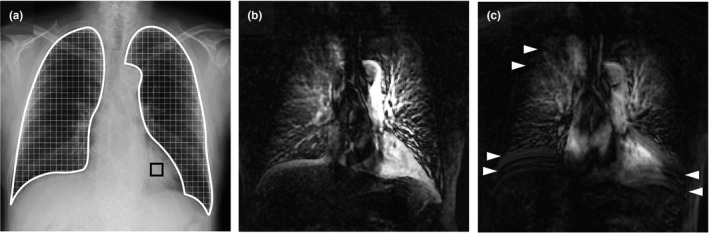
Pulmonary perfusion images and respiratory artifacts in chest digital dynamic radiography (DDR). A 74‐yr‐old male with chronic obstructive pulmonary disease. (a) Original chest radiography. The edges of the lung fields (white frame region) and the region of interest (10 × 10 mm) in the left ventricle (black frame box) were automatically determined. The lung fields were separated using 5‐mm intervals, and changes in the pixel value of each block were analyzed. (b) Maximum intensity projection (MIP) image for chest DDR using the breath‐holding protocol. Excursion of the right diaphragm was 1.6 mm. Entrance surface dose was 1.18 mGy. The mean correlation rates of the bilateral lung fields were 38.7% (right) and 46.6% (left). (c) MIP image for chest DDR using the deep‐breathing protocol. Excursion of the right diaphragm was 2.0 mm. Entrance surface dose was 1.83 mGy. The mean correlation rates of the bilateral lung fields were 30.4% (right) and 35.6% (left). Pulmonary perfusion of the bilateral lower lung fields became vague (blurred image) with the deep‐breathing protocol vs the breath‐holding protocol. Horizontal lines observed in the lung field (white arrowhead) were regarded as incomplete pause of the diaphragm and ribs (misalignment of the rib cage).