
Figure 3. Indications for right heart catheterization (RHC).
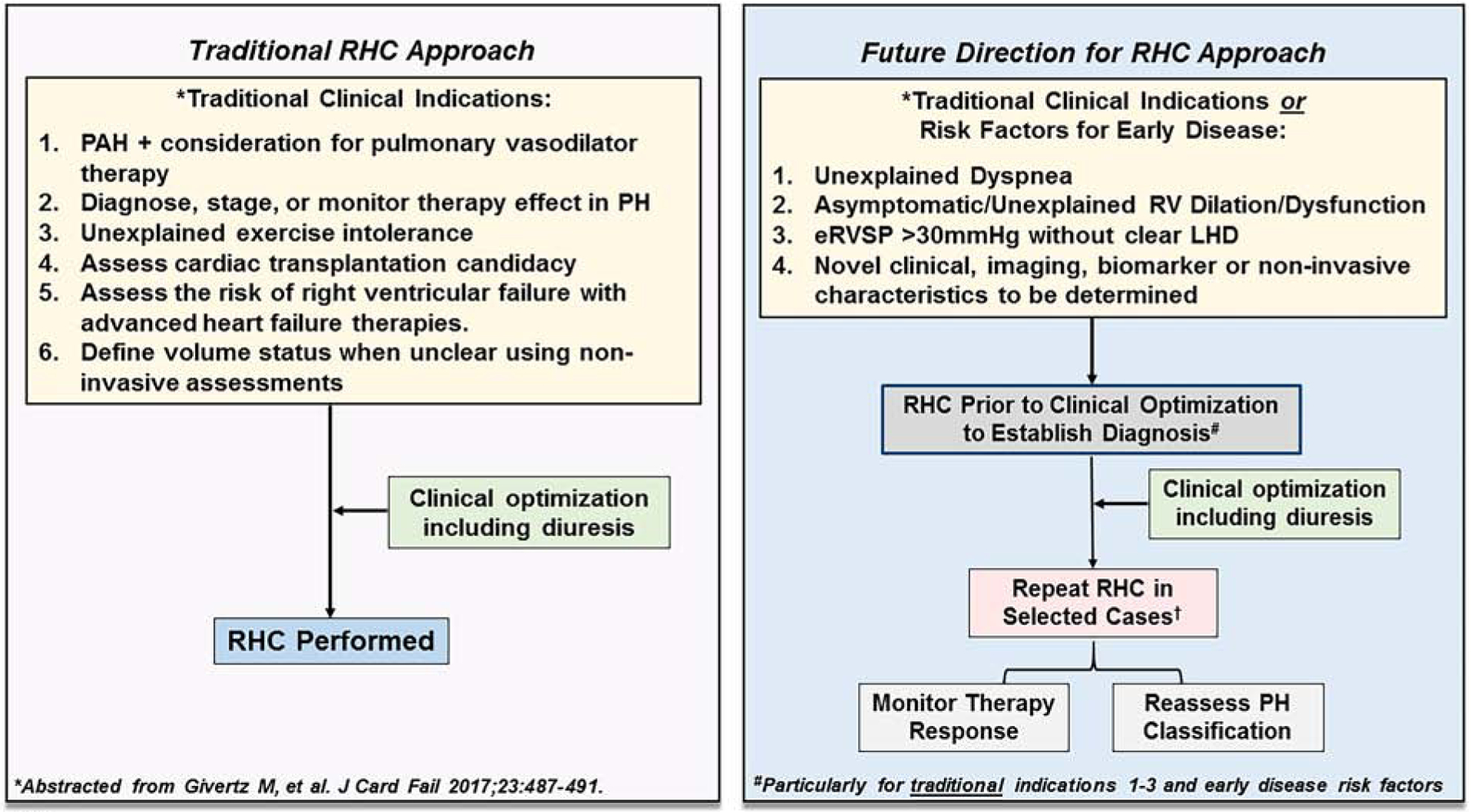
(Left) In the traditional approach to RHC, hemodynamic assessment is performed in patients with a clinical indication following clinical optimization including diuresis. PAH, pulmonary arterial hypertension. (Right) A future direction for RHC approach considers patients with a traditional indication for RHC as well as patients with clinical parameters suggestive of early or unexplained pulmonary hypertension (PH). In this scenario, RHC prior to diuresis may be considered to clarify the PH hemodynamic classification of patients (particularly post-capillary PH vs. combined pre- and post-capillary PH). In select patients, repeat RHC may be indicated to monitor therapy response or reassess PH hemodynamic classification. Unexplained dyspnea is dyspnea without a clear etiology based on results from standard non-invasive testing (e.g., echocardiography, cardiopulmonary exercise testing, others); eRVSP, estimated right ventricular systolic pressure by echocardiography; LHD, left heart disease.